|
|






 Arabic
Arabic Bengali
Bengali Chinese
Chinese English
English French
French German
German Hebrew
Hebrew Hindi
Hindi Italian
Italian Japanese
Japanese Korean
Korean Malay
Malay Polish
Polish Portuguese
Portuguese Spanish
Spanish Turkish
Turkish Ukrainian
Ukrainian Vietnamese
Vietnamese|
Lecture notes, cheat sheets
Anesthesiology and resuscitation. Basic manipulations in intensive care (lecture notes)
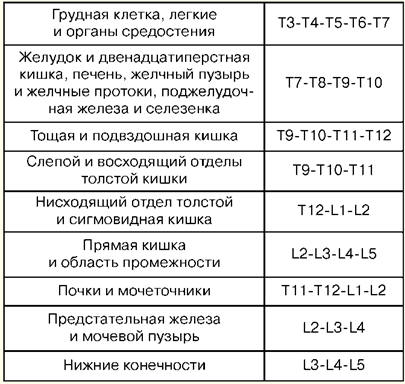
Directory / Lecture notes, cheat sheets Table of contents (expand) Lecture number 2. Basic manipulations in intensive care Percutaneous puncture and catheterization of the main vein (subclavian). Indications: large volumes of infusion-transfusion therapy, parenteral nutrition, detoxification therapy, intravenous antibiotic therapy, cardiac probing and contrast, measurement of central venous pressure, implantation of a pacemaker, impossibility of catheterization of peripheral veins. Contraindications: violation of the blood coagulation system, inflammatory and purulent process at the site of puncture and catheterization, trauma in the clavicle area, superior vena cava syndrome, Paget-Schretter syndrome. Instruments and accessories for puncture and catheterization: puncture needle, set of plastic catheters, set of conductors, 10 ml syringe for intramuscular injections, scissors, needle holder, surgical needle and silk ligature, adhesive plaster. Technique. Catheterization is carried out in compliance with the rules of asepsis and antisepsis, cleaning the operator’s hands, the surgical field and covering with sterile material. The patient's position is horizontal on his back with his arms brought to the body and his head turned in the opposite direction. Local anesthesia is used - 0,5-1% solution of novocaine. It is better to perform the puncture on the right, since when puncturing the left subclavian vein there is a danger of damaging the thoracic lymphatic duct. The puncture point is on the border of the inner and middle third of the clavicle, 2 cm below it. The needle is passed slowly at an angle of 45° to the collarbone and 30-40° to the surface of the chest between the collarbone and the first rib in the direction of the upper edge of the sternoclavicular joint. When passing the needle, the syringe piston is periodically pulled up to determine whether it has entered the vein, and novocaine is injected along the needle. When a vein is pierced, there is sometimes a sinking feeling. After entering the vein, the syringe is disconnected from the needle and the cannula is closed with a finger. Then a guidewire is inserted through the needle to a length of 15-20 cm and the needle is removed. A catheter of the appropriate diameter is passed along the conductor and, together with the conductor, is inserted into the vein 6-8 cm, after which the conductor is carefully removed. To check that the catheter is positioned correctly, a syringe is attached to it and 2-3 ml of blood is drawn into it, after which a plug is placed or infusion therapy is started. The catheter is fixed to the skin with a silk ligature. To do this, a sleeve is made from an adhesive plaster on the catheter 3-5 mm from the skin, on which silk is tied, then passed through the ears of the catheter and tied again. After fixing the catheter, the puncture site is covered with an aseptic sticker. Complications: puncture of the subclavian artery, air embolism, puncture of the pleural cavity, damage to the brachial plexus, damage to the thoracic lymphatic duct, damage to the trachea, thymus and thyroid gland, suppuration at the puncture site. 1. Tracheostomy Indications: obstruction of the larynx and upper trachea due to obstruction by a tumor or foreign body, paralysis and spasm of the vocal cords, severe swelling of the larynx, acute respiratory distress, aspiration of vomit, prevention of asphyxia in severe chest injuries. Instrumentation: 2 scalpels, 2 anatomical and surgical tweezers each, several hemostatic clamps, an elevator, a grooved probe, 2 blunt and 1 single-tooth sharp hook, a Trousseau or Deschamps dilator, surgical needles with a needle holder. Technique The patient lies on his back, with a cushion under his shoulders, and his head thrown back. If the patient is in a state of asphyxia, the cushion is placed only at the last moment, before opening the trachea. Local infiltration anesthesia is performed with a 0,5-1% solution of novocaine with the addition of adrenaline. In case of acute asphyxia, surgery can be performed without anesthesia. Identification points: the angle of the thyroid cartilage and the tubercle of the cricoid cartilage. An incision in the skin, subcutaneous tissue and superficial fascia is made from the lower edge of the thyroid cartilage to the jugular notch strictly along the midline of the neck. The median vein of the neck is pushed back or ligated, finding the linea alba, along which the muscles are bluntly pushed apart and the isthmus of the thyroid gland is exposed. The edges of the incision are spread apart with a Trousseau dilator, ligatures are applied to the edge of the wound and a tracheostomy tube is carefully inserted, making sure that its end enters the lumen of the trachea. The surgical wound is sutured. The tube is fixed on the patient’s neck with a gauze splint, previously tied to the shield of the tube. The inner tube is inserted into the outer tube. 2. Conicotomy The patient is placed on his back with a transverse bolster at the level of the shoulder blades. The patient's head is tilted back. After treating the skin on the front surface of the neck with an antiseptic solution, the larynx is fixed with fingers on the lateral surfaces of the thyroid cartilage and the gap between the thyroid and cricoid cartilage, where the cone ligament is located, is felt. Under local infiltration anesthesia, a transverse skin incision about 2 cm long is made with a pointed scalpel, the cone-shaped ligament is felt and it is dissected or perforated. Any tracheostomy cannula of suitable diameter is inserted into the resulting hole and secured with a gauze strip around the neck. If a cannula is not available, it can be replaced with a piece of rubber or plastic tube of suitable diameter and length. To prevent this tube from slipping inside the trachea, its outer end at a distance of 2 cm from the edge is pierced in the transverse direction and fixed with a gauze strip. Konicotomes are a metal tracheostomy cannula of small diameter with a piercing mandrel inside it. After dissecting the skin over the cone-shaped ligament, it is pierced with a conicotome, the mandrin is removed, and the cannula is installed in a position that ensures free flow of air into the trachea and secured. In extreme cases, with obstruction of the entrance to the larynx and a sharp disruption of the airway, it can be restored by inserting 1-2 thick needles with an internal diameter of 2-2,5 mm into the trachea in the midline below the level of the thyroid cartilage. The needles are inserted at an acute angle to the axis of the trachea, sometimes without local anesthesia, to a depth of 1-1,5-2 cm. The characteristic sound of air escaping during respiratory movement and a decrease in the manifestations of respiratory failure indicate the effectiveness of such an emergency measure until the airway is optimally maintained. . 3. Puncture of the pleural cavity Indications: severely difficult breathing due to compression of the lungs by massive effusion in pleurisy or hydrothorax, as well as air in valvular pneumothorax. Technique The puncture is performed in a sitting position, under aseptic conditions. To anesthetize the puncture site, use a 0,5% solution of novocaine. For puncture, a thick needle connected to a rubber tube is used. The puncture is made along the upper edge of the rib, since the intercostal vessels are located along the lower edge. The penetration of a needle into the pleural cavity is felt as a “failure into the void.” Aspiration of fluid along the needle confirms that the tip of the needle is in the pleural cavity. Each time when separating a filled syringe from a rubber tube, the latter must be clamped with a hemostatic clamp to prevent atmospheric air from being sucked into the pleural cavity. After aspiration is completed, an aseptic bandage is applied to the puncture site. Complications: injury to the intercostal artery, vessels of the lung diaphragm, puncture of the stomach or intestines. Tracheal intubation. Indications: narrowing of the larynx, pathological breathing, acute respiratory failure, coma II and III degrees, high risk of aspiration during surgical interventions on the thoracic and abdominal organs, head and neck, diseases of the pharynx, larynx and trachea (acute inflammation, cancer, tuberculosis and etc.). A laryngoscope is used for intubation. It consists of a handle and a blade. Curved blades are most widely used, as they are more physiological. Straight blades are used for long necks. Preparation for intubation includes checking equipment and positioning the patient correctly. The endotracheal tube should be checked. The cuff is tested by inflating it using a 10 ml syringe. Check the contact of the blade with the laryngoscope handle and the light bulb. It is necessary to ensure that suction is ready in case of sudden sputum discharge, bleeding or vomiting. Successful intubation depends on the correct positioning of the patient. The patient's head should be located at the level of the intubating xiphoid process. Moderate elevation of the head while simultaneously extending the atlanto-occipital joint creates an improved position for intubation. Preparation for intubation also includes mandatory pre-oxygenation. The laryngoscope is taken in the non-dominant hand (for most people this is the left), and the patient's mouth is opened wide with the other hand. The blade is inserted along the right side of the oropharynx, avoiding damage to the teeth. The tongue moves to the left, and the blade is raised upward, towards the vault of the pharynx. The tip of the curved blade is inserted into the vallecula (a hole located on the anterior surface of the epiglottis), while the tip of the straight blade should be used to lift the epiglottis directly. The laryngoscope handle is moved up and forward perpendicular to the lower jaw until the vocal cords come into view. Reliance on teeth should be avoided. The endotracheal tube is taken in the right hand and passed through the open glottis under visual control. The cuff should be located in the upper parts of the trachea, but below the larynx. The laryngoscope is removed from the mouth, again avoiding damage to the teeth. Immediately after intubation, auscultation is performed over the lungs on both sides (since it is possible to pass the tube into one bronchus) and in the epigastrium (to exclude intubation of the esophagus). If the tube is in the trachea, it is secured in the desired position with ribbons and the cuff is inflated. The cuff should be placed above the level of the cricoid cartilage, since its prolonged placement in the larynx can lead to hoarseness in the postoperative period. Complications: intubation of the esophagus, bronchus, placement of the cuff in the larynx, dental damage, dislocation of the lower jaw, laryngospasm, reflex disorders (hypertension, tachycardia, increased intracranial pressure), respiratory tract injury, inflammation, etc. 4. Puncture and catheterization of the epidural space Indications: severe pain, surgical interventions, providing postoperative analgesia. The level of placement of the epidural block depends on which organ needs to be anesthetized. Table No. 1 shows examples of “target organs” during epidural puncture. Table 1 Levels of the spinal column and "target organs"
Instrumentation: anesthesia needles, a special needle for puncture of the epidural space, a sample syringe, a catheter, a plug, filter balls, napkins, adhesive tape and sterile gloves. Position the patient sitting or lying on his side. In this case, the knees and chin should be brought as close to the chest as possible. In this way, maximum flexion of the spine is created, at which the angle between the spinous processes of adjacent vertebrae increases and the approach to the ligamentum flavum is facilitated. Under aseptic conditions and under local anesthesia with a 0,5% solution of novocaine, a puncture of the epidural space is performed. The needle is inserted strictly perpendicularly, but with osteochondrosis, an angle of inclination or puncture in the midthoracic region is possible. When the needle enters the thickness of the ligaments, the mandrel is removed from it and a syringe with liquid is attached. Further advancement of the needle is done slowly and smoothly with pressure on the syringe piston. Due to the significant resistance of the ligaments, the liquid cannot leave the syringe. Disconnect the syringe and insert the catheter 5-7 cm; there should be no resistance. The needle is removed and the conductor is fixed to the back with an adhesive plaster, bringing it to the anterior surface of the chest. The plug with the filter is fixed to the conductor. An anesthetic is administered. Afterwards the level of skin anesthesia is determined. Complications: respiratory and hemodynamic disorders, intoxication, damage to the dura mater, neurological complications, periduritis. 5. Lumbar puncture Indications: presence of meningeal syndrome, high intracranial pressure, differential diagnosis between ischemic and hemorrhagic stroke, traumatic brain injury, spinal cord tumors. Contraindications: the presence of an inflammatory or purulent process at the puncture site, hemorrhagic diathesis, tumor of the posterior cranial fossa, dislocation of the trunk, terminal condition of the patient, with blurred boundaries of the optic nerve. The puncture point is between the 3rd and 4th spinous processes of the lumbar vertebrae. The manipulation is carried out under aseptic conditions, under local anesthesia. The needle goes perpendicular towards the navel. The patient's position is the same as for an epidural puncture. When passing three ligaments (external and internal interspinous, yellow ligament), a feeling of failure occurs, the mandrel is removed from the needle, and cerebrospinal fluid appears. After taking the cerebrospinal fluid for examination, a mandrel is inserted and the needle is removed, and an aseptic sticker is applied. Unlike epidural puncture, damage to the dura mater occurs. Cerebrospinal fluid is transparent, colorless, pressure 100-200 mmH0,33O. Art., protein content 1003 g/l, HC - 1008-7,35, pH = 7,40-2, sugar content equal to half of blood sugar (normally 3-110 mmol/l), chlorides - 120-5 mmol/l, cell count up to XNUMX lymphocytes. Complications: epiduritis, dislocation of the brain into the foramen magnum, neurological disorders. Author: Kolesnikova M.A. << Back: The concept of resuscitation >> Forward: Acute disturbances of consciousness
▪ History of Economic Thought. Lecture notes ▪ Fundamentals of life safety. Crib ▪ Introduction to pedagogical activity. Crib
The existence of an entropy rule for quantum entanglement has been proven
09.05.2024 Mini air conditioner Sony Reon Pocket 5
09.05.2024 Energy from space for Starship
08.05.2024
▪ Space Rider Orbital Laboratory ▪ Qi technology for wireless battery charging ▪ The Gulf Stream slowed down due to global warming ▪ Transistor of one molecule and several atoms ▪ White sharks make animals stressed
▪ section of the site Sites of amateur radio equipment. Article selection ▪ article by Erich Maria Remarque. Famous aphorisms ▪ What animal children are four times the size of their parents? Detailed answer ▪ article Yacht from a kayak. Personal transport ▪ article Measuring mini-laboratory. Encyclopedia of radio electronics and electrical engineering ▪ article UHF amplifier from SKD-1. Encyclopedia of radio electronics and electrical engineering
Home page | Library | Articles | Website map | Site Reviews
www.diagram.com.ua |


 See other articles Section
See other articles Section 