|
|






 Arabic
Arabic Bengali
Bengali Chinese
Chinese English
English French
French German
German Hebrew
Hebrew Hindi
Hindi Italian
Italian Japanese
Japanese Korean
Korean Malay
Malay Polish
Polish Portuguese
Portuguese Spanish
Spanish Turkish
Turkish Ukrainian
Ukrainian Vietnamese
Vietnamese|
Lecture notes, cheat sheets
Anesthesiology and resuscitation. Artificial ventilation (lecture notes)
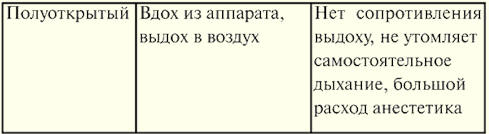
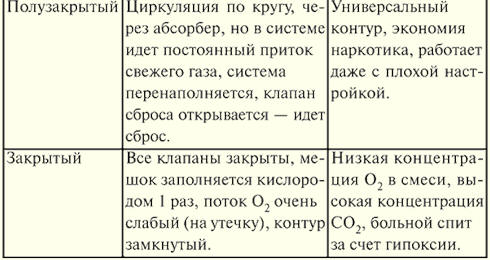
Directory / Lecture notes, cheat sheets Table of contents (expand) Lecture number 15. Artificial lung ventilation Artificial lung ventilation (ALV) provides gas exchange between the surrounding air (or a certain mixture of gases) and the alveoli of the lungs, is used as a means of resuscitation in the event of a sudden cessation of breathing, as a component of anesthesia and as a means of intensive care for acute respiratory failure, as well as some diseases of the nervous and muscular systems. Modern methods of artificial lung ventilation (ALV) can be divided into simple and hardware. A simple method of mechanical ventilation is usually used in emergency situations (apnea, with an abnormal rhythm, agonal breathing, with increasing hypoxemia and (or) hypercapnia, and severe metabolic disorders). The expiratory methods of IVL (artificial respiration) from mouth to mouth and from mouth to nose are simple. Hardware methods are used if necessary for long-term mechanical ventilation (from one hour to several months and even years). The Phase-50 respirator has great potential. For pediatric practice, the apparatus "Vita-1" is produced. The respirator is connected to the patient's airways through an endotracheal tube or tracheostomy cannula. Hardware ventilation is carried out in the normal frequency mode, which ranges from 12 to 20 cycles per 1 min. In practice, there are mechanical ventilation in high-frequency mode (more than 60 cycles per 1 min), in which the tidal volume decreases markedly (up to 150 ml or less), positive pressure in the lungs at the end of inspiration decreases, as well as intrathoracic pressure, and blood flow to the heart improves. Also, in high-frequency mode, the patient's adaptation to the respirator is facilitated. There are three methods of high-frequency ventilation: volumetric, oscillatory and jet. Volume is usually carried out with a respiratory rate of 80-100 per 1 min, oscillatory IVL - 600-3600 per 1 min, which ensures the vibration of a continuous or intermittent gas flow. The most widespread jet high-frequency ventilation with a respiratory rate of 100-300 per minute, in which a jet of oxygen at a pressure of 1-2 atm is blown into the airways through a needle or catheter with a diameter of 2-4 mm. Jet ventilation is carried out through an endotracheal tube or tracheostomy (at the same time, atmospheric air is sucked into the respiratory tract) and through a catheter that is inserted into the trachea through the nasal passage or percutaneously (puncture). The latter is important in situations where there are no conditions for tracheal intubation. Artificial ventilation of the lungs can be carried out in automatic mode, but this is acceptable in cases where the patient's spontaneous breathing is completely absent or suppressed by pharmacological drugs (muscle relaxants). Assisted ventilation is also carried out, but in this case, the patient's independent breathing is preserved. Gas is supplied after the patient makes a weak attempt to inhale, or the patient is synchronized to an individually selected mode of operation of the apparatus. There is also an Intermittent Mandatory Ventilation (PMV) mode, which is applied during the gradual transition from mechanical ventilation to spontaneous breathing. In this case, the patient breathes on his own, but additionally, a continuous flow of the gas mixture is supplied to the airways. Against this background, with a specified frequency (from 10 to 1 time per minute), the device performs an artificial breath, coinciding (synchronized PVL) or not coinciding (non-synchronized PVL) with the patient's independent inspiration. The gradual reduction of artificial breaths allows you to prepare the patient for spontaneous breathing. Breathing circuits are shown in Table 10. Table 10 Breathing circuits
Manual ventilation with a bag or mask is readily available and is often sufficient to adequately inflate the lungs. Its success, as a rule, is determined by the correct selection of the size of the mask and the experience of the operator, and not by the severity of the lung pathology. Показания 1. Resuscitation and preparation of the patient in a short period of time for subsequent intubation. 2. Periodic ventilation with a bag and mask to prevent post-extubation atelectasis. 3. Restrictions on ventilation with a bag and a mask. Equipment A conventional breathing bag and a mask with an installed pressure gauge or a self-inflating breathing bag with an oxygen chamber are used. Techniques for conducting 1. It is necessary to place the mask tightly on the patient's face, giving the patient's head a median position with the chin fixed with a finger. The mask should not lie on the eyes. 2. Respiratory rate - usually 30-50 per 1 min. 3. Inspiratory pressure - usually 20-30 cm of water. Art. 4. Greater pressure (30-60 cm of water column) is acceptable during primary resuscitation in the labor activity of a woman. Efficiency mark 1. Return of heart rate to normal numbers and the disappearance of central cyanosis. 2. Excursion of the chest should be good, breathing is carried out equally well on both sides. 3. The study of the gas composition of the blood is usually required and carried out during prolonged resuscitation. Complications 1. Pneumothorax. 2. Bloating. 3. Hypoventilation syndrome or episodes of apnea. 4. Irritation of the skin of the face. 5. Retinal detachment (when applying a mask to the eyes and creating a long-term high peak pressure). 6. Mask and bag ventilation may worsen the patient's condition if he actively resists the procedure. Hardware IVL Показания 1. Apnea. 2. Coma in the acute period, even without signs of respiratory failure. 3. Seizures not controlled by standard anticonvulsant therapy. 4. Shock of any etiology. 5. Increase in the dynamics of the syndrome of CNS depression in hyperventilation syndrome. 6. With a birth spinal injury in newborns - the appearance of forced breathing and crepitating widespread wheezing against the background of shortness of breath. 7. RO2 capillary blood less than 50 mm Hg. Art. during spontaneous breathing with a mixture with FiO2 0,6 or more. 8. RSO2 capillary blood more than 60 mm Hg. Art. or less than 35 mm Hg. Art. with spontaneous breathing. Equipment: "PHASE-5", "BP-2001", "Infant-Star 100 or 200", "Sechrist 100 or 200", "Babylog 1", "Stephan", etc. Principles of treatment 1. Oxygenation in stiff lungs can be achieved by increasing the inspired oxygen concentration, increasing the inspiratory pressure, increasing the PEEP, prolonging the inspiratory time, increasing the plateau pressure. 2. Ventilation (removal of CO2) can be enhanced by an increase in tidal volume, an increase in frequency, and a prolongation of expiratory time. 3. The selection of ventilation parameters (frequency, inspiratory pressure, inspiratory plateau, inspiratory-expiratory ratio, PEEP) will vary depending on the nature of the underlying disease and the patient's response to therapy. Purposes of IVL 1. Oxygen: reach pO2 50-100 mmHg Art. 2. Hold pCO2 within 35-45 mm Hg. Art. 3. Exceptions: in some situations, pO indicators2 and pCO2 may differ from the above: 1) in chronic pulmonary pathology, higher pCO values2 portable; 2) with severe heart defects, smaller pO numbers are tolerated2; 3) depending on the therapeutic approach in the case of pulmonary hypertension, larger or smaller pCO values are tolerated2. 4. Indications and ventilation parameters should always be documented. Techniques for conducting 1. Initial parameters of IVL: inspiratory pressure 20-24 cm of water. Art.; PEER from 4-6 cm of water. Art.; respiratory rate 16-24 per 1 min, inhalation time 0,4-0,6 s, DO from 6 to 10 l / min, MOV (minute ventilation volume) 450-600 ml / min. 2. Synchronization with a respirator. As a rule, patients are synchronous with the respirator. But excitement can impair synchronization, in such cases, drug therapy (morphine, promedol, sodium oxybutyrate, muscle relaxants) may be required. Examination 1. An important component of the survey are repeated blood gas tests. 2. Physical examination. Control of the adequacy of the IVL. When performing emergency ventilation with a simple method, it is enough to observe the color of the skin and movements of the patient's chest. The chest wall should expand with each inhalation and fall with each exhalation, but if the epigastric region rises, then the blown air enters the esophagus and stomach. The reason is often the wrong position of the head of the patient. When conducting long-term mechanical ventilation, it is necessary to judge its adequacy. If the patient's spontaneous breathing is not suppressed by pharmacological preparations, then one of the main signs of the adequacy of the IVL performed is the good adaptation of the patient to the respirator. In the presence of a clear consciousness, the patient should not have a feeling of lack of air, discomfort. Breath sounds in the lungs should be the same on both sides, and the skin should have a normal color. Complications 1. The most common complications of mechanical ventilation are: rupture of the alveoli with the development of interstitial emphysema, pneumothorax and pneumomediastinitis. 2. Other complications can be: bacterial contamination and infection, obturation of the endotracheal tube or extubation, one-lung intubation, pneumopericarditis with cardiac tamponade, decreased venous return and decreased cardiac output, chronicity of the process in the lungs, stenosis and obstruction of the trachea. Against the background of mechanical ventilation, it is possible to use a number of analgesics, which should provide a sufficient level and depth of anesthesia in doses, the introduction of which under conditions of spontaneous breathing would be accompanied by hypoxemia. By maintaining a good supply of oxygen to the blood, mechanical ventilation contributes to the fact that the body copes with the surgical injury. In many operations on the organs of the chest (lungs, esophagus), separate bronchial intubation is used, which makes it possible to turn off one lung from ventilation during surgical interventions in order to facilitate the work of the surgeon. Such intubation also prevents the contents from the operated lung from flowing into the healthy lung. During operations on the larynx and respiratory tract, transcatheter jet high-frequency ventilation is used, which facilitates the examination of the surgical field and allows maintaining adequate gas exchange with the trachea and bronchi opened. Under conditions of general anesthesia and muscle relaxation, the patient is not able to respond to the resulting hypoxia and hypoventilation, therefore, it is important to control the blood gas content (continuous monitoring of oxygen partial pressure and carbon dioxide partial pressure) by percutaneous means using special sensors. In case of clinical death or agony, mechanical ventilation is a mandatory component of resuscitation. It is possible to stop carrying out mechanical ventilation only after the consciousness is completely restored and spontaneous breathing is complete. In the complex of intensive care, mechanical ventilation is the most effective method for the treatment of acute respiratory failure. It is carried out through a tube that is inserted into the trachea through the lower nasal passage or tracheostomy. Of particular importance is the care of the respiratory tract, their adequate drainage. Auxiliary mechanical ventilation is used in sessions for 30-40 minutes to treat patients with chronic respiratory failure. IVL is used in patients in a state of coma (trauma, brain surgery), as well as with peripheral damage to the respiratory muscles (polyradiculoneuritis, spinal cord injury, amyotrophic lateral sclerosis). ALV is also widely used in the treatment of patients with chest trauma, various poisonings, cerebrovascular accidents, tetanus, and botulism. Author: Kolesnikova M.A. << Back: Patient severity assessment and monitoring >> Forward: Infuzionnaya therapy (Blood transfusion. Parenteral nutrition)
▪ History of religion. Lecture notes
The existence of an entropy rule for quantum entanglement has been proven
09.05.2024 Mini air conditioner Sony Reon Pocket 5
09.05.2024 Energy from space for Starship
08.05.2024
▪ Self-guided loader Seegrid GP8 Series ▪ LG to launch phone with flexible OLED display ▪ 60V and 75V MOSFETs for Synchronous Rectification Circuits ▪ Discovered a unique mineral from the Earth's mantle ▪ Why do dinosaurs have a long neck
▪ section of the Radio Control website. Article selection ▪ article Man is a wolf to man. Popular expression ▪ article What ruins wine? Detailed answer ▪ Article Blood pressure and its measurement. Health care ▪ article Triac control unit. Encyclopedia of radio electronics and electrical engineering ▪ article Invisible coin. Focus Secret
Home page | Library | Articles | Website map | Site Reviews
www.diagram.com.ua |


 See other articles Section
See other articles Section 