|
|






 Arabic
Arabic Bengali
Bengali Chinese
Chinese English
English French
French German
German Hebrew
Hebrew Hindi
Hindi Italian
Italian Japanese
Japanese Korean
Korean Malay
Malay Polish
Polish Portuguese
Portuguese Spanish
Spanish Turkish
Turkish Ukrainian
Ukrainian Vietnamese
Vietnamese|
Lecture notes, cheat sheets
Internal illnesses. Cheat sheet: briefly, the most important
Directory / Lecture notes, cheat sheets Table of contents
1. THE SUBJECT OF INTERNAL DISEASES, HISTORY AND OBJECTIVES Internal diseases is a field of clinical medicine that studies the etiology, pathogenesis, semiotics, treatment, prognosis and prevention of diseases of internal organs. Internal medicine is the most important section of practical medicine, covering most human diseases. The term "internal diseases" came into practice in the XNUMXth century. and supplanted the more general term "therapy". From the point of view of a clinician, any disease is a change in the normal functioning of the body, characterized by a violation of the functional activity of a particular system, a limitation of the adaptive, compensatory and reserve capabilities of the body and a decrease in its ability to work. Disease is a dynamic process, in which dynamism is determined by the coexistence of damage and repair reactions. The ratio between these reactions reflects the direction of the disease towards either recovery or progression. Elucidation of this direction makes it possible to assess the outcome of the disease, to predict the fate of the patient. Diagnosis of a disease (from the Greek. diagnosis - "recognition") - a brief definition of the essence of the pathological process, reflecting the cause of its occurrence, the main mechanisms that led to the development of changes in the body, and the characteristics of these changes. Each diagnosis that the doctor makes is a differential diagnosis, weighing each individual symptom, evaluating and differentiating it. In the early stages of development, medicine was not a science and was purely empirical knowledge based only on observations. For the first time, a representative of ancient Greek medicine, Hippocrates, when examining a patient, used palpation, listening, and compiled a description of many symptoms and syndromes of diseases. The doctrine of the pulse was created by the representative of the Alexandrian school Herophilus, the description of some signs of pleurisy, stomach ulcers, meningitis was presented by the Tajik scientist Abu-Ali Ibn-Sina (Avicenna). In the XVIII-XIX centuries. questions of internal medicine were developed in detail by Auenbrugger, Laennek, G. I. Sokolsky, M. Ya. Mudrov, G. A. Zakharyin. The scientific clinical school of internal medicine was created by S. P. Botkin, subsequently developed by many brilliant clinicians: I. M. Sechenov, V. P. Obraztsov, N. D. Strazhesko, B. E. Votchal, A. M. Myasnikov, N S. Molchanov, E. M. Tareev, V. Kh. Vasilenko, etc. At the present stage of development of internal medicine, a great contribution was made by domestic scientists E. I. Chazov, P. E. Lukomsky, F. I. Komarov, G. I. Dorofeev, A. G. Chuchalin, A. I. Vorobyov and others. The final diagnosis of the disease should include information about the etiology (etiological diagnosis), its pathogenesis (pathogenetic diagnosis), morphological changes (morphological diagnosis) and functional state (functional diagnosis) of the affected organ or system. The final diagnostic formula accumulates all types of diagnoses, and reflects the doctor's view of the pathological process by highlighting the underlying disease, complications and concomitant diseases. In the future, the doctor determines the direction of the development of the pathological process, possible outcomes and consequences of the disease. The assessment of all these changes is carried out as a result of observation of the patient, the use of special additional studies, the treatment used. 2. NEUROCIRCULATORY ASTHENIA (ETIOLOGY, PATHOGENESIS, CLASSIFICATION, CLINIC) Neurocirculatory asthenia is a functional disease, which is based on a failure of adaptation or a violation of the neuroendocrine regulation of the cardiovascular system. Etiology. The reasons for development can be external and internal factors. External factors: psycho-emotional, physical overstrain, violation of the regime of work and rest. Internal factors: congenital or acquired inferiority of the nervous and humoral systems of regulation of vascular tone, features of the protective and adaptive mechanisms of the body (such as higher nervous activity, the state of the endocrine system). Pathogenesis. The formation of the disease occurs against the background of a genetic or acquired inferiority of the neurohormonal system. There is a formation of neurosis and visceral disorders, while the internal organs are involved in emotional arousal selectively. With an increase in the activity of the sympathoadrenal system and a relative decrease in the activity of the cholinergic system, the formation of hypertensive and cardiac types of NCA occurs. With an increase in the activity of the cholinergic system and a relative insufficiency of the sympathoadrenal system, the formation of the hypotensive type of NCA occurs. Classification. In the clinic, the most common classification of NCA according to Z. N. Savitsky (1956) and V. P. Nikitin (1957) with the following types: cardiac, hypertensive, hypotensive, mixed. Clinic. Main syndromes: neurotic, cardiac (algic or arrhythmic variants), hypertonic, hypotonic, respiratory disorders syndrome, hyperkinetic, asthenic, vascular. It is characterized by the presence of a large number of various subjective signs of the disease. There are complaints of pain in the region of the heart, which are localized in the region of the apex of the heart, have a dull, aching, stabbing character. There may be a feeling of heaviness and pressure. Pain is often associated with excitement and emotional stress, can be short-term or long-term. They can radiate to the left arm and shoulder blade of the left shoulder, they are not removed by nitroglycerin, which is poorly tolerated by anyone. Complaints that characterize respiratory distress include periodic deep breaths, frequent shallow breathing, leading to a state of hyperventilation (dizziness, blackouts). There may be sensations of heat, hot flashes to the head, a short-term fainting state. Acrocyanosis, sweating, pronounced red or white dermographism, "games" of vasomotors of the skin. There may be signs of peripheral circulatory disorders (such as Raynaud's syndrome), temperature asymmetries, lability of the pulse, blood pressure, a tendency to tachycardia, respiratory arrhythmia due to dysfunction of the respiratory center, extrasystole, group extrasystoles, attacks of paroxysmal tachycardia. There are general weakness, fatigue, irritability, headache, unstable sleep, a tendency to rapid mood swings. Distracted attention, memory loss, dizziness, a feeling of fear are noted. The boundaries of the heart do not change, the tones are clear, a functional systolic murmur can be heard at the apex, associated with an acceleration of blood flow and a change in the tone of the capillary muscles. The nature of the noise changes with a change in body position, decreases or disappears with physical activity. 3. NEUROCIRCULATORY ASTHENIA (MAIN TYPES, DIAGNOSIS, COMPLICATIONS, TREATMENT) The type of NCA is formed depending on the nature and severity of dysfunctions of the sympathoadrenal and cholinergic systems, as well as on the relationship between adreno- and cholinergic processes. The dynamics of changes in blood pressure depends on the type of NCA. For NCA by cardiac type are characteristic: persistent sinus (sometimes paroxysmal) tachycardia, extrasystole, an increase in minute blood volume. Severe tachycardia and a decrease in pulse pressure are noted during functional tests (orthostatic and with physical activity). NCA of the hypertensive type is characterized by: lability of blood pressure with a tendency to systolic hypertension, an increase in stroke and minute blood volumes, good tolerability of an orthostatic test with an increase in average hemodynamic pressure. NCA of the hypotensive type is characterized by fainting or collapsed states, lability of blood pressure with a tendency to hypotension, muffled heart sounds, increased cardiac output, poor tolerance of an orthostatic test with a drop in average hemodynamic pressure, tachycardia, an increase in minute blood volume during physical activity (immediately after its end, a sharp decrease in blood pressure is possible). Arterial hypotension is considered pressure numbers: at the age of 25 years - 100/60 mm Hg. Art. and less, over the age of 30 - below 105/65 mm Hg. Art. Diagnostic research. Of diagnostic importance are studies of the level of catecholamines in the blood and urine, 17-hydroxycorticosteroids (increase in quantity), estrogen levels (decrease in quantity), and the study of thyroid function. Indicators of central hemodynamics: with the cardiac type, there is an increase in cardiac output and a decrease in specific peripheral resistance, the average hemodynamic pressure remains unchanged. Blood pressure indicators are examined with the determination of residual and basal pressure. The average hemodynamic pressure is investigated - it is measured by the tachiooscillographic method. Functional stress tests are used: Master's test, step test, bicycle ergometry in cardiac NCA, dosed physical activity test, hyperventilation test, breath holding test. If there are negative T waves on the ECG, stress pharmacological tests are performed: a test with inderal, potassium chloride, atropine, and adrenaline. The ECG may reveal: sinus tachycardia, bradycardia and arrhythmia, impaired atrioventricular conduction, displacement of the RS-T segment below the isoelectric line, flattening and appearance of a negative T wave, ventricular extrasystoles. Complications. Arrhythmia, acute vascular insufficiency (fainting, collapse), autonomic crises, angioedema. Treatment. Elimination of etiological factors, rehabilitation of hidden foci of chronic infection. Sedatives according to indications, hypnotics are used only for severe sleep disorders. Tranquilizers are used in small doses, short courses. β-blockers are used for the hypertensive type of NCA with tachycardia. Forecast. The prognosis is favorable, performance is restored. 4. HYPERTENSION (ETIOLOGY, PATHOGENESIS, CLASSIFICATION, CLINIC) A chronically occurring disease, the main manifestation of which is the syndrome of arterial hypertension, not associated with the presence of pathological processes in which an increase in blood pressure is due to known causes. Etiology. Neuropsychic overstrain, dysfunction of the sex glands. Pathogenesis. There is a violation of the biosynthesis of sympathetic amines, as a result of which the tone of the sympathetic-adrenal system increases. Against this background, the activation of the pressor mechanisms of the renin-angiotensin-aldosterone system and the inhibition of depressor factors: prostaglandins A, E, and the kinin system occur. Classification. In clinical conditions, the disease is divided according to the severity of arterial hypertension, the degree of risk of developing damage in target organs, and the stage of development of hypertension. Clinic. With stage I hypertension, periodic headaches, tinnitus, and sleep disturbance appear. Mental performance decreases, dizziness, nosebleeds are noted. Possible cardialgia. In the left thoracic branches, the presence of high-amplitude and symmetrical T waves is possible, the minute volume of the heart remains normal, increasing only during exercise. Hypertension crises develop as an exception. With stage II hypertension, frequent headaches, dizziness, shortness of breath during exercise, and sometimes angina attacks appear. Nocturia and the development of hypertensive crises are possible. The left border of the heart shifts to the left, at the apex the first sound is weakened, an accent of the second tone is heard above the aorta, sometimes a pendulum-like rhythm. With stage III hypertension, two options are possible: 1) development of vascular accidents in target organs; 2) a significant decrease in minute and stroke volumes of the heart with a high level of peripheral resistance. In the malignant form of hypertension, extremely high blood pressure figures are noted (diastolic blood pressure exceeds 120 mmHg). Renal failure progresses, vision decreases, weight loss, symptoms from the central nervous system, changes in the rheological properties of the blood appear. hypertensive crises. Sudden sharp increase in blood pressure. Crises are of two types. Type I crisis (hyperkinetic) is short-term. It manifests itself as a sharp headache, dizziness, decreased vision, nausea, and less often vomiting. Characterized by agitation, palpitations and trembling throughout the body, pollakiuria; towards the end of the crisis, polyuria or profuse loose stools are observed. Systolic blood pressure increases and pulse pressure increases. Type II crisis (eu- and hypokinetic) is severe. It develops gradually, lasting from several hours to 4-5 days or more. Caused by circulatory hypoxia of the brain, characteristic of later stages of hypertension. It manifests itself as heaviness in the head, sharp headaches, sometimes paresthesia, focal disturbances of cerebral circulation, and aphasia. There may be anginal pain in the heart area, vomiting, and attacks of cardiac asthma. Diastolic pressure increases significantly. Blood pressure must be reduced gradually over several hours. 5. HYPERFOLIC DISEASE (DIAGNOSIS, TREATMENT, PROGNOSIS, PREVENTION) Diagnostic research. The examination includes 2 stages: a mandatory study and a study to assess the damage to target organs. Mandatory studies: general blood and urine analysis, determination of potassium, fasting glucose, creatinine, total blood cholesterol, electrocardiography, chest x-ray, fundus examination, ultrasound examination of the abdominal organs. Additional studies: echocardiography, ultrasound examination of peripheral vessels, determination of the lipid spectrum and triglyceride levels. Complications. Hemorrhagic stroke, heart failure, III-IV degree retinopathy, nephrosclerosis, angina pectoris, myocardial infarction, atherosclerotic cardiosclerosis. Differential diagnosis. Secondary hypertension: diseases of the kidneys, adrenal glands (Itsenko-Cushing syndrome, Conn syndrome), pheochromocytoma, Itsenko-Cushing disease, organic lesions of the nervous system, hemodynamic arterial hypertension (coarctation of the aorta, aortic valve insufficiency, sleep-disordered breathing syndrome), iatrogenic arterial hypertension . Treatment. At high and very high risk levels, immediate medication is prescribed. If the patient is classified as a medium risk group, the question of treatment is taken by the doctor. It is possible to observe with control over blood pressure from several weeks to 3-6 months. Drug therapy should be initiated while maintaining blood pressure levels above 140/90 mm Hg. Art. In the low-risk group, longer follow-up is possible - up to 6-12 months. Drug therapy is prescribed while maintaining blood pressure levels of more than 150/95 mm Hg. Art. Non-drug treatments include smoking cessation, weight loss, alcohol restriction, increased physical activity, and reduced salt intake to 5 g per day. Effective drug combinations: 1) diuretic and b-blocker; 2) a diuretic and an ACE inhibitor or an angiotensin II receptor antagonist; 3) a calcium antagonist from the group of dihydropyridones and a β-blocker; 4) calcium antagonist and ACE inhibitor; 5) a-blocker and b-blocker; 6) a drug of central action and a diuretic. In case of uncomplicated hypertensive crisis, treatment can be carried out on an outpatient basis, b-blockers, calcium antagonists (nifedipine), short-acting ACE inhibitors, loop diuretics, prazosin are prescribed orally. With a complicated hypertensive crisis, vasodilators (sodium nitroprusside, nitroglycerin, enaprilat), antiadrenergic drugs (phentolamine), diuretics (furosemide), ganglioblockers (pentamine), antipsychotics (droperidol) are administered parenterally. Flow. Long-term, with periods of remission. Forecast. At stage I - favorable, at stages - serious. Prevention. Treatment of patients with neurocirculatory dystonia, monitoring of persons at risk, use of active recreation. When a diagnosis of hypertension is made, continuous comprehensive treatment is carried out. 6. MYOCARDITIS Myocarditis is an inflammatory disease of the heart muscle of an infectious, allergic or toxic-allergic nature. Etiology. Main factors: bacterial infections, purulent-septic diseases, viral infection, allergic factors, intoxication. Pathogenesis. Myocardial damage leads to the development of dystrophic-necrobiotic changes in muscle cells. Clinic. The main clinical variants: pain (not accompanied by heart failure, recovery after 1-2 months), arrhythmic (with severe myocardial damage), circulatory failure (severe diffuse myocardial damage in combination with rhythm and conduction disorders), mixed (pain with arrhythmic, arrhythmic with circulatory failure, etc.), Abramov-Zidler. The disease begins during the period of convalescence or 1-2 weeks after recovery from infection. An inexplicable low-grade fever appears, rarely - fever, weakness, malaise, sweating. Objectively, tachycardia, low pulse filling, and in severe cases an alternating pulse are noted. In severe cases, the size of the heart increases, blood pressure is normal or reduced. Heart sounds are muffled, splitting of the first sound is possible, a muscle systolic murmur appears above the apex of the heart, and there may be a pericardial friction murmur. With Abramov-Fiedler's myocarditis, increasing symptoms of progressive heart failure, thromboembolism of the kidneys, lungs, and spleen suddenly appear. Diagnostic research. A general blood test is performed (leukocytosis, increased ESR). Biochemical study (dysproteinemia, an increase in the content of a- and b-globulins, an increase in the level of sialic acids, the appearance of C-reactive protein, an increase in the activity of AST and CPK in severe forms), a virological study, an immunological study. An ECG study reveals: ST segment displacement, T wave changes - flat, biphasic, negative, QRST complex expansion, voltage decrease. Flow. It can be acute, abortive, recurrent, latent, chronic. Complications. Arrhythmias, circulatory failure, angina pectoris, myocardial cardiosclerosis, thromboembolism. Differential diagnosis. Should be carried out with neurocirculatory dystonia, coronary heart disease, thyrotoxic myocardial dystrophy, primary rheumatic carditis. Treatment. Appointment of bed rest. Conducted etiotropic therapy, which is effective in infectious myocarditis, with viral myocarditis is ineffective. Symptomatic therapy is carried out with cardiac glycosides, antiarrhythmic drugs, diuretics, metabolic agents. Forecast. With most myocarditis, the prognosis is favorable, with Abramov-Fiedler myocarditis - serious. Prevention. Primary measures for the prevention of the disease: timely treatment and sanitation of foci of infections. Secondary prevention - dispensary dynamic monitoring of ill persons. 7. INFECTIOUS ENDOCARDITIS A peculiar form of sepsis, characterized by the localization of the pathogen on the heart valves or parietal endocardium, followed by damage to many organs and systems. Etiology. Pathogens: cocci, gram-negative bacteria, fungi such as Candida, rickettsia, viruses, Brucella. Risk factors: acquired and congenital heart defects, minor surgical and dental operations, parenteral drug administration, prosthetic heart valves, urinary tract infection, prolonged use of catheters, abortions, program hemodialysis. Classification. Taken into account: 1) clinical and morphological form: primary (on unchanged valves) and secondary (against the background of rheumatic, syphilitic, atherosclerotic, defects, arteriovenous aneurysms, prosthetic valves); 2) the nature of the course (acute, subacute, chronic (recurrent)); 3) the degree of activity of the process: I degree - minimal, II degree - moderate, III degree - high. Clinic. The main manifestations of the disease: fever (from subfebrile to high), accompanied by chills, profuse sweating, muscle weakness, muscle and joint pain, loss of appetite. The skin is pale with an icteric tint, petechial rashes, especially on the skin of the lower eyelid (Lukin-Libman symptom), painful nodules on the palms and soles (Osler's nodes). Fingers in the form of drumsticks, nails - watch glasses. Tachycardia, muffled heart sounds, rhythm and conduction disturbances, which is typical for developing myocarditis. systolic murmur over the aorta due to narrowing of the aortic orifice. Occurs a few weeks after the onset of the disease. With the development of aortic insufficiency, diastolic murmur appears over the aorta. Diagnostic research. Complete blood count (anemia, leukopenia, thrombocytopenia, increased ESR). Biochemical blood test - dysproteinemia, hypergammaglobulinemia, positive formol test. Immunological study - inhibition of the non-specific link of the immune response, activation of the humoral link (increase in IgA, IgM, CEC). Bacteriological examination of blood (triple blood cultures). With an ECG - a violation of the rhythm and conduction, a decrease in the voltage of the teeth. Echocardiography: the presence of vegetations on the cusps of the affected valve, signs of a formed heart disease, ruptures of chords, perforation of the cusps. Complications. Infarction of the lungs, myocardium, kidneys, pulmonary edema, heart failure, embolic disorders of cerebral circulation of the spleen, retinal vessels. Treatment. Administration of the antistaphylococcal penicillinase-resistant antibiotic oxacillin, 2 g every 4 hours (12 g/day). Prednisolone (40-60 mg / day), non-steroidal anti-inflammatory drugs. Cardiac glycosides, potassium preparations, diuretics, for anemia - iron preparations in combination with vitamins B and C in the dystrophic phase. Flow. In the acute form it is rapidly progressive, in the subacute form it is protracted, in the chronic form it is recurrent. Forecast. In the acute form, the prognosis is relatively favorable; in subacute and chronic forms, the prognosis is relatively favorable. Prevention. Prevention of the development of bacterial infections, active treatment of acute infections. 8. PERICARDITIS Pericarditis is an inflammatory disease of the pericardium, which is more often a local manifestation of a certain disease (tuberculosis, rheumatism, diffuse connective tissue diseases) or a concomitant disease of the myocardium and endocardium. Etiology. They are caused by bacteria, viruses, fungi, rickettsiae, mycobacteria, typhoid and dysentery bacillus. Aseptic pericarditis with allergies, systemic lesions of the connective tissue, traumatic injuries, autoimmune processes. There is a group of idiopathic pericarditis. Pathogenesis. The infection penetrates into the pericardial cavity by the hematogenous or lymphogenous route. Exudative processes intensify. The accumulation of a large amount of exudate in the pericardial cavity is manifested by the syndrome of cardiac tamponade. Clinic. With dry (fibrinous) pericarditis: pain in the region of the heart of varying strength, a pericardial friction rub is heard, more often it is determined on the sternum and to the left of the parasternal line, it is heard in any phase of the cardiac cycle. It has a scratchy tint, can last for several hours or months. With effusion (exudative) pericarditis: shortness of breath, cough (usually dry), vomiting is possible. The body temperature rises, the boundaries of the heart increase in all directions, the apex beat decreases or disappears, the cervical veins swell. With a large effusion, the pulse decreases, blood pressure decreases. With cardiac tamponade: severe chest pain, collapse, tachycardia, paradoxical pulse. With compression of the superior vena cava, the formation of a "consular" head, Stokes collar. With compression of the inferior vena cava: hepatomegaly, premature ascites, Breitman's position, periodic disturbance of consciousness. With adhesive (adhesive) pericarditis: pain in the region of the heart, dry cough, retraction of the apex beat (symptom of Sali-Chudnovsky). On auscultation, the three-term nature of the rhythm, the appearance of systolic non-conductive noise over the anterior surface of the heart. With constrictive (compressive) pericarditis: in the early stages of shortness of breath, slight cyanosis of the lips and tip of the nose. In the advanced stage, Beck's triad: high venous pressure, ascites, "small quiet heart." Neck veins swell, face puffiness, cyanosis. The position of the patient in orthopnea. trophic disorders. The apex beat disappears. Atrial fibrillation, arterial pressure is reduced, venous pressure is increased. Possible low systolic murmur, marked anasarca, hydrothorax, ascites. Diagnostic research. Complete blood count, (leukocytosis with a shift of the formula to the left, an increase in ESR), ECG studies, EchoCG studies. Treatment. In the acute period, bed rest, diet. Etiotropic therapy. NSAIDs (not indicated for secondary pericarditis, myocardial infarction), glucocorticoids for 1-1,5 months (not prescribed for tumors), antihistamines, vitamin C. With squeezing pericarditis, surgical treatment. Flow. Acute (passes within 1-2 months), long-term, progressive. Forecast. In acute forms it is often favorable, in chronic forms it is serious. 9. RHEUMATISM (SOKOLSKY-BUYO DISEASE) (ETIOLOGY, PATHOGENESIS, CLINIC, DIAGNOSIS) Rheumatism is a systemic toxic-immunological inflammatory disease of connective tissue with a predominant localization of the process in the cardiovascular system. Etiology. The disease is caused by group A beta-hemolytic streptococcus. Pathogenesis. Released streptococcal antigens (streptolysin-O, streptokinase, streptohyaluronidase) lead to the development of the acute phase of inflammation by cellular exudation and phagocytosis. Chronic inflammation gradually develops with the transfer of activity to immune mechanisms, collagen formation with the formation of fibrosis processes. Classification. According to Nesterov A.I. (1990), the following are taken into account: 1) the phase of the disease (active or inactive, specifying the degree of activity of the process - minimal, medium, high); 2) clinical and anatomical characteristics of damage to the heart and other organs; 3) the nature of the course of the disease (acute, subacute, protracted, continuously relapsing, latent); 4) the state of blood circulation (0, I, Na, Nb, III degree of violations). Clinic. The first period of pre-rheumatism lasts 2-4 weeks from the end of streptococcal infection to the onset of manifestations of the disease. Appear: malaise, fatigue, loss of appetite, palpitations, tingling in the joints, hyperhidrosis, pallor of the skin. The second represents a rheumatic attack. Fever appears with syndromes of damage to the joints, heart (primary rheumatic heart disease) and other organs. The third period of clinical manifestations. There is recurrent rheumatic heart disease with progressive heart damage, the formation of complex heart defects. Primary rheumatic heart disease. Inflammation of all membranes of the heart (pancarditis) is possible, the endocardium and myocardium are most often affected. There is tachycardia, rarely bradycardia. The borders of the heart are normal or moderately enlarged. Auscultation muffled I tone, soft systolic murmur at the apex (associated with myocarditis). Sometimes a third tone may appear. Diagnostic criteria for rheumatism according to Kisel-Jones. Major criteria: carditis, polyarthritis, chorea, annular erythema, subcutaneous rheumatic nodules. Minor criteria: previous rheumatism, arthralgia, fever, increased ESR, increased C-reactive protein, leukocytosis, prolongation of the PQ interval on the ECG, increased titer of anti-streptococcal antibodies in the blood, detection of streptococcal antigen. If two major and one or two minor criteria are present, the diagnosis is considered reliable; if one major and two minor criteria are present, the diagnosis is considered probable. Diagnostic research. Diagnostic value is the study of a complete blood count (hypochromic anemia, leukocytosis with a shift to the left, an increase in ESR), a biochemical blood test (the appearance of C-reactive protein, an increase in fibrinogen, dysproteinemia, a2-hyperglobulinemia, an increase in the content of hap2 toglobin, ceruloplasmin, acid phosphatase ). An immunological study is being carried out to determine the increase in the titer of antibodies ASH, ASL-O, ASA, myocardial antibodies. ECG determines various rhythm disturbances, conduction, Doppler echocardiography determines structural changes. 10. RHEUMATISM (SOKOLSKY-BUYO DISEASE) (DIFFERENTIAL DIAGNOSIS, TREATMENT, PROGNOSIS, PREVENTION) Differential diagnosis. Infectious myocarditis develops at the height of the infection, it is not characterized by progression, signs of valvulitis. Of the connective tissue diseases, it is necessary to take into account periarteritis nodosa, systemic lupus erythematosus, scleroderma. With neurocircular dystonia of the cardiac type, there are diverse complaints, there are no objective signs of the disease. In the syndrome of primary tuberculosis, there are no radiographic symptoms of the primary complex, antistreptococcal antibodies. Mantoux and Pirquet tests are carried out, tuberculosis mycobacteria in sputum are examined. Treatment. With active rheumatism, mandatory hospitalization is carried out up to 40-60 days or more. An appropriate regimen is assigned: in the absence of carditis - half-bed for 7-10 days, then free; in the presence of carditis - strict bed rest for 2-3 weeks, then semi-bed and free. From nutrition, table No. 10 is prescribed with a protein content of at least 1 g / kg, limiting salt to 6 g / day. Mandatory early prescription of antibiotics is carried out: benzylpenicillin 1,5-4 million units per day (depending on the degree of activity) for 2 weeks. Then they switch to a prolonged form: bicillin-5, 1,5 million units every 2 weeks for 2 months. After this, antibiotic therapy is carried out every 3 weeks every month for at least 3 years in patients without a history of carditis and for at least 5 years in patients with a history of carditis. If you are allergic to penicillin, antibacterial drugs of other groups are used - macrolides, oral cephalosporins. Glucocorticoid drugs are prescribed only for severe carditis, acute (less often subacute) course of the disease: prednisolone 20-30 mg / day for 2-3 weeks, then the dose is reduced until the drug is completely discontinued, the course of treatment is 1,5-2 months. Of the metabolic drugs, phosphalene, a polarizing mixture and antiarrhythmic drugs (for arrhythmias) are used. With the development of circulatory failure, saluretics are used: hypothiazide, furosemide, uregit, ACE antagonists in a short course. Flow. If the duration of the disease is up to 6 months, it is considered as acute, more than 6 months - chronic. Forecast. Determined by the condition of the heart. The absence of signs of clinical formation of defects within 6 months is a good prognostic indicator. The formation of a defect within 6 months is considered to be an unfavorable prognostic sign. Prevention. Primary prevention includes hardening children from the first months of life, nutritious nutrition, physical education and sports, improving living conditions, timely treatment and sanitation of foci of streptococcal infection. Secondary prevention in patients who have had the first rheumatic attack without carditis is more effective until the age of 18, in patients with carditis with the first attack of rheumatism it is more effective until the age of 25. In patients with valvular disease, bicillinoprophylaxis can be carried out throughout life. 11. MITRAL VALVE PROLAPSE A condition characterized by prolapse of one or both leaflets of the mitral valve into the cavity of the left atrium, which usually occurs in the second half of ventricular systole (in the exile phase). Prolapse means "bulging". Etiology. Congenital forms are noted in the syndromes of Marfan, Emre-Danlos, Holt-Oram-pa, atrial septal defect, Ebstein's anomaly, Fallot's tetrade. Acquired forms are observed in coronary heart disease, rheumatism, neurocirculatory dystonia, hypertrophic cardiomyopathy, thyrotoxicosis, and chest injuries. Pathogenesis. During ventricular systole, blood flows not only into the aorta, but partially back into the left atrium. Classification. In a clinical setting, mitral valve prolapse is divided into: 1) according to the severity (I - prolapse 3-6 mm, II - prolapse 6-9 mm, III - prolapse more than 9 mm); 2) according to the degree of regurgitation (semi-quantitative assessment in points (1-4)); 3) downstream (mild, moderate, severe, asymptomatic (18%)). Clinic. There are syncope with lipothymia (a feeling of fear of death), palpitations, interruptions in the work of the heart, stabbing, pressing pains in the heart, shortness of breath. There are: weakness, fatigue, headache, stabbing pains in the region of the heart, palpitations, fluctuations in blood pressure, dizziness, fainting. Accompanying signs: narrow shoulder girdle, thin elongated bones, elongated fingers with increased mobility of the joints of the hands, elongated nails, hypomastia in women, unexpressed hair on the chest in men, blond hair, gray-blue eyes. A typical systolic click and late systolic murmur are auscultated. To determine, it is necessary to conduct a test with physical activity or nitroglycerin. Diagnostic study. ECG study: identifying signs of repolarization disorders, ST wave depression in II, III, aVF, left precordial leads, T wave inversion, rhythm and conduction disturbances. Conducted phonocardiographic study, Holter ECG monitoring for 24-48 hours, echocardiography, angiography of the left heart, functional tests with physical activity or nitroglycerin to determine the degree of tolerance. Flow. In asymptomatic and mild cases, the disease proceeds for a long time, without progression; in moderate and severe cases, it lasts for a long time, with progression. Differential diagnosis. Anomalies in the development of the mitral valve, additional leaflets (up to 3-4), additional chord. Treatment. In asymptomatic cases, periodic examinations every 2-3 years are necessary. b-blockers are used in medium dosages. Antibiotic therapy before minor and major surgical interventions. Antiarrhythmic drugs A (quinidine, procainamide) for supraventricular rhythm disturbances and group B (mexiletine, toclenide) for ventricular arrhythmias. Forecast. With an uncomplicated course - favorable, with a complicated course - serious. 12. MITRAL VALVE DEFECTS Mitral valve insufficiency - incomplete closure of the valves during left ventricular systole as a result of damage to the valvular apparatus. Etiology. Organic lesions of the valve leaflets or chords in atherosclerosis, rheumatism (up to 75%), infective endocarditis, diffuse connective tissue diseases, less often in visceral forms of rheumatoid arthritis. Pathogenesis. As a result of incomplete closure of the mitral valve leaflets, a reverse flow of blood occurs during systole from the left ventricle into the left atrium. Tonogenic dilatation and hypertrophy of the left atrium occurs. The left atrium loses muscle tone and its pressure increases. Passive (venous) pulmonary hypertension occurs. Clinic. Enlargement of the borders of the heart in all directions. At the first stage, the valve defect is compensated, no complaints are made. With the development of passive (venous) pulmonary hypertension with stagnation in the pulmonary circulation, shortness of breath, attacks of cardiac asthma appear, which ends with the formation of right ventricular failure. Diagnostic study. ECG examination, X-ray examination, echoCG examination, Doppler echocardiography examination. Treatment. Conservative treatment is carried out with the underlying disease and heart failure. Surgical treatment involves mitral valve replacement. Forecast. With the development of heart failure - unfavorable. Mitral stenosis is a narrowing of the left atrioventricular orifice, which obstructs the movement of blood from the left atrium to the left ventricle. Etiology. Organic lesions (rheumatism), congenital malformations (Lutembashe syndrome - mitral). Pathogenesis. Fusion of the mitral valve leaflets and tendon threads along the free edge. The area of the mitral orifice decreases (normally 4-6 cm2). Hypertrophy and tonogenic dilatation of the left atrium develop, and systole lengthens. Clinic. Patients have an asthenic build, are infantile, the skin is pale, and there is facial cyanosis (facies mitralis). Shortness of breath, weakness, palpitations, occasional cough, sometimes hemoptysis, suffocation at night, and occasionally dysphonia and dysphagia appear. The borders of the heart are enlarged upward and to the right, a flapping 1st sound, presystolic murmur, bifurcation of the 2nd tone, “cat purring”, weak, irregular pulse are heard. Diagnostic study. ECG examination, X-ray examination, echoCG examination. Complications. Congestion in the pulmonary circulation, hemoptysis, cardiac asthma, high pulmonary hypertension, pulmonary aneurysm, dilatation of the heart cavities, atrial fibrillation and flutter, thromboembolism, spherical thrombus in the left atrium, symptoms of compression (recurrent nerve, subclavian artery). Treatment. More often performed: mitral comis-surotomy. Symptomatic therapy is carried out with circulatory failure and an active rheumatic process. Forecast. With timely commissurotomy and subsequent active antirheumatic therapy - favorable. 13. VALVAL VALVES OF THE AORTIC Aortic valve insufficiency is the incomplete closure of the semilunar cusps of the aortic valve, which leads to a backflow of blood from the aorta into the left ventricle during its diastole (aortic regurgitation). Men are more often ill. Etiology. Rheumatism, atherosclerosis, infective endocarditis, syphilitic mesaortitis, congenital anomalies, diffuse connective tissue diseases, and injuries are important. Pathogenesis. As a result of incomplete closure of the aortic valve cusps in diastole, blood flows back from the aorta into the cavity of the left ventricle. There comes a volumetric diastolic overload of the left ventricle, its hypertrophy. Clinic. There are no clinical manifestations in the compensation stage. In the stage of circulatory insufficiency, pulsation of large arteries, "carotid dance", Musset's symptom, positive capillary pulse, pulsation of pupils, dizziness, fainting, pain in the heart area are noted. Cyanosis is pronounced, the borders of the heart are enlarged to the left. A diastolic murmur is heard in the second intercostal space on the left, and an enlarged, painful liver is palpated. Shortness of breath and suffocation occur in the stage of decompensation. Diagnostic study. ECG examination, X-ray examination, Doppler echocardiography examination, echocardiography examination. Treatment. Cardiac glycosides are used, prescribed with caution due to slowing heart rate and increasing cardiac output, vasodilators to deposit blood in the vascular system and reduce regurgitation. During surgical treatment, aortic valve replacement is performed. Flow. In the stage of compensation, the course is long, in the stage of decompensation it is rapidly progressing. Forecast. With timely treatment - relatively favorable. Aortic stenosis is a heart disease caused by narrowing of the aortic ostium. It is rare in isolated form, more often in combination with aortic valve insufficiency. Most often men are ill. Etiology. Valvular narrowing of the aorta with rheumatism, atherosclerosis, infective endocarditis, gummous syphilis, congenital narrowing of the aortic orifice, or subvalvular (subaortic) narrowing with hypertrophy of the interventricular septum. Pathogenesis. As a result of the narrowing of the aortic orifice, the systole time of the left ventricle is prolonged. Clinic. There are no clinical manifestations in the compensation stage. With physical exertion, emotional stress, pain in the region of the heart (like angina pectoris), shortness of breath, dizziness, a tendency to faint, and headache may appear. With a decrease in the contractile function of the left ventricle, attacks of cardiac asthma may occur. Diagnostic study. ECG examination, X-ray examination, echoCG examination. Treatment. Treatment of the underlying disease, angina pectoris (nitrates, calcium channel blockers), heart failure. Surgical treatment - aortic commissurotomy, aortic valve replacement. Forecast. Under compensated conditions - favorable. 14. INSUFFICIENCY OF THE THREE-LEAVEL VALVE Leaflet valve insufficiency is incomplete closure of the valve leaflets, as a result of which part of the blood flows from the right ventricle into the right atrium during systole. Valve insufficiency can be absolute or relative. In the first case, the cause of the disorder is damage to the tricuspid valve and its leaflets. The cause of relative insufficiency is damage to the muscle of the right ventricle, as a result of which the valve ring is stretched. Relative tricuspid valve insufficiency occurs 3 times more often than organic insufficiency. Etiology. In the development of the disease, the following are important: organic failure (rheumatism, infective endocarditis) and relative failure with severe dilatation of the right ventricle (mitral stenosis, pulmonary hypertension, cardiosclerosis, pneumosclerosis). Pathogenesis. During contraction of the right ventricle, part of the blood returns to the right atrium, which simultaneously receives the usual amount of blood from the vena cava. Dilatation of the right atrium occurs with excess blood flow in diastole into the right ventricle, dilatation and hypertrophy of the right ventricle). Decompensation of venous congestion in the systemic circulation develops early. Clinic. Clinical manifestations of signs of insufficiency of the right side of the heart are characterized by moderate shortness of breath during physical exertion, which does not sharply limit activity (as with mitral stenosis), there is no difficulty in breathing in the supine position. There are: weakness, palpitations, vague pain in the heart, heaviness in the right hypochondrium, dyspeptic disorders, drowsiness, edema. Expressed cyanosis of the skin and visible mucous membranes (sometimes with an icteric tinge), swelling and pulsation of the jugular veins (positive venous pulse), right ventricular heart beat, epigastric pulsation, pulsation of the liver, anasarca, ascites. The borders of the heart are enlarged only to the right. Systolic murmur, better auscultated by the right border of the heart, increases with inspiration, there is no emphasis on the pulmonary artery, arterial pressure is reduced, venous pressure is increased. Additional diagnostic study. An ECG study shows a rightogram, a negative T wave in II, III standard leads, right chest leads, signs of right atrial hypertrophy, atrial fibrillation, incomplete blockade of the right bundle branch block. X-ray examination establishes a significant increase in the right ventricle and right atrium, there are no changes in the pulmonary pattern. In the FCG study in the 5th intercostal space on the right and left of the sternum, immediately after the first tone, a systolic murmur is determined, occupying the entire systole; at the height of forced inspiration with breath holding, its severity increases. EchoCG study reveals an increase in the amplitude of the opening of the anterior leaflet, dilatation of the cavity of the right ventricle, hyperkinesia of its walls. Treatment. Used conservative treatment and preventive treatment of congestive circulatory failure. Forecast. With congestive circulatory failure, the prognosis is poor. 15. ATHEROSCLEROSIS A disease of the body, the pathomorphological substrate of which is the accumulation of lipids in the inner and middle membranes of large and medium-sized arteries, followed by the deposition of calcium salts, the development of scar connective tissue. Etiology and pathogenesis. Impaired lipid metabolism leads to changes in metabolism and permeability of the vascular wall. On the surface of the vascular wall, the formation of atherosclerotic plaques occurs, their ulceration, and the formation of thrombotic masses on the ulcerated surfaces. Secondary deposition of calcium salts occurs in the plaques themselves. The main types of dyslipoproteinemia (according to G.F. Fredrikson): 1) type 1: increased chylomicron fraction, no risk of atherosclerosis; 2) type 2a: increased LDL fraction, high risk of atherosclerosis; 3) type 2b: increased fractions of LDL, VLDL (very low density), the risk of atherosclerosis is very high; 4) type 3: increased LPPP fractions (intermediate density); 5) type 4: increased VLDL fraction; 6) type 5: increased fractions of VLDL and chylomicrons. Clinic. In type 1, eruptive xanthomas, retinal lipid infiltration, recurrent pancreatitis, and hepatosplenomegaly are noted. In type 2a, there are: lipoid corneal arch, tuberculate and tendon xanthomas, xanthelasmas. In type 2b, there are: lipoid corneal arch, xanthelasma, hyperuricemia, impaired glucose tolerance. Type 3 has palmar xanthomas, tuberculate xanthomas. Type 4 has recurrent pancreatitis. Type 5 has xanthomas, dyspnea, hepatosplenomegaly. Diagnostic research. To determine the type of dyslipoproteinemia, a biochemical study is carried out on the levels of triglycerides, total cholesterol, HDL. Protein metabolism is being studied (dysproteinemia, decrease in albumin, increase in g-globulin in the sclerotic stage of the course of the disease). Treatment. Lifestyle change. It is necessary to follow a diet, exercise, monitor body weight, stop smoking. Initially, diet 1 is prescribed according to nutritional recommendations for atherosclerosis. In the presence of predisposing factors for the development of atherosclerosis, a more rigid diet is prescribed 2 - with familial hypercholesterolemia, the presence of coronary artery disease (coronary heart disease), with the ineffectiveness of the first stage diet. Antioxidants, fish oil are used. Carrying out drug therapy involves taking anion-exchange resins, HMG-CoA reductase inhibitors (statins), nicotinic acid, niacinamide, drugs of the fibric acid group, drugs with antioxidant properties. In severe hypertriglyceridemia, plasmapheresis is indicated. Forecast. Serious, especially with damage to the coronary vessels, cerebral vessels, kidneys. Prevention. In primary prevention, it is necessary to use the regulation of diet, expand physical activity. In secondary prevention, an annual determination of the lipid profile is used. 16. ISCHEMIC HEART DISEASE. ANGINA Ischemic heart disease is myocardial damage caused by a disorder of the coronary circulation, resulting from an imbalance between the coronary blood flow and the metabolic needs of the heart muscle. Etiology. Atherosclerosis of the coronary arteries, vasospasm, disturbances in the hemostasis system, an underdeveloped network of collateral circulation, hyperproduction of catecholamines are of primary importance. Pathogenesis. With angina pectoris, there is a discrepancy between the blood supply to the myocardium and its needs, the development of ischemia. Clinic With the first occurrence of angina pectoris, a pain syndrome lasting less than 1 month is characteristic. With stable angina pectoris of functional class I, the pain syndrome occurs during accelerated walking or walking with an average step of up to 1000 m (VEM (veloergometry) - 750 kgm / min. With stable angina of the II functional class, the pain syndrome occurs when walking on flat terrain up to 500 m (VEM - 450 kgm / min). With stable angina of functional class III, the pain syndrome occurs when walking on flat terrain up to 150-200 m (VEM - 150-300 kgm / min). With stable angina of the IV functional class, there is an inability to perform any load without the onset of an angina attack (VEM is not performed). Progressive angina is characterized by a sudden increase in the frequency and duration of attacks with the same degree of physical activity. Spontaneous (vasospastic or Prinzmetal's variant) angina occurs at night. With angina pectoris, pain is more often localized behind the sternum with irradiation to the left arm, shoulder blade, neck, sometimes to the left half of the jaw, has a compressive burning character, pain duration from 5-10 minutes to 25-30 minutes. Possible bradycardia or tachycardia, rise in blood pressure. Diagnostic research. A biochemical blood test, an ECG study, coronary angiography, stress tests or pharmacological tests, an echocardiogram study are carried out. Treatment. Pain is relieved with nitroglycerin. Drug treatment includes the use of long-acting nitrates, nitrate-like agents - nitrong, sustak, sustanite, nitrosorbitol, sydnopharm, erinite. Calcium antagonists are used cordafen, corinfar, verapamil. Of the β-blockers, atenolol, metaprolol (egilok), nebivolol (nebilet), etc. are used. Antiarrhythmic drugs, antispasmodics (if indicated), anabolic agents, prodectin are used. Surgical treatment includes coronary artery bypass grafting, percutaneous transluminal angioplasty. Flow. With angina pectoris, the course is undulating, depending on the degree and progression of atherosclerosis of the coronary arteries. Forecast. With angina pectoris, the prognosis depends on the severity of atherosclerosis of the coronary arteries, on the frequency of angina attacks. Prevention. Primary prevention includes the following activities: identification of risk factors, rational organization of the regime of work and rest. Secondary prevention includes dispensary observation of persons with unstable forms of angina pectoris, arterial hypertension. 17. ISCHEMIC HEART DISEASE. MYOCARDIAL INFARCTION Pathogenesis. With myocardial infarction, insufficient blood supply to the myocardium occurs with the development of lesions and necrosis in it. Clinic. The first period of myocardial infarction represents the period of precursors (prodromal). New-onset angina may occur, the most acute period lasts up to 2 hours. The duration of the acute period is up to 8-10 days, the following course options are available: 1) anginal (pain behind the sternum for more than 20 minutes), motor restlessness, cold sticky sweat, nausea and vomiting; 2) gastralgic (pain in the epigastric region); 3) asthmatic (acute left ventricular failure); 4) arrhythmic (acute rhythm disturbances); 5) cerebral (insufficiency of cerebral circulation); 6) asymptomatic (lack of clinical manifestations). This is followed by a subacute period lasting up to 4-8 weeks. Then a post-infarction period develops, lasting up to 2-6 weeks. The pain syndrome differs in intensity, duration (from several hours to a day or more). The pain has a pressing, compressive, cutting, tearing character, is localized more often behind the sternum, less often captures the entire anterior chest wall. The pain radiates to the left shoulder, arm, sometimes jaw, epigastric region, is not removed by nitroglycerin, sometimes by drugs. Patients are excited, experience fear of death. The skin is pale, the mucous membranes are cyanotic, bradycardia develops, more often moderate tachycardia, a short-term increase in blood pressure. Heart sounds are weakened, a proto-diastolic gallop rhythm can be heard. Diagnostic study. Manifestations of resorption-necrotic syndrome are noted (an increase in the level of leukocytes in prephyseal blood on the first day, after 2-3 days an increase in ESR with a gradual decrease in the number of leukocytes). The levels of transaminases specific for myocardial infarction are studied: myoglobin, microfraction of creatine kinase (MB-CK mass) - early markers of myocarditis damage; troponin, microfraction of creatine kinase (CF-CK) - late markers of myocarditis damage. It is necessary to take into account the de Ritis coefficient (AST/ALT ratio), which increases to more than 1,33 with myocardial damage. In myocardial infarction, an ECG study shows a pathological Q wave with a depth of more than 1/3 R and a width of more than 0,03, there is a shift in the ST interval upward from the isoline and negative T. Treatment. Pain relief is carried out with narcotic analgesics, fentanyl with droperidol, nitrous oxide anesthesia, and epidural anesthesia. If the pain syndrome lasts less than 6 hours, thrombolytic and anticoagulant therapy is performed. Nitrates, β-blockers are used to prevent an increase in the necrosis zone. In the subacute period, long-acting nitrates, indirect anticoagulants are used to strengthen the coronary circulation. Flow. It can be uncomplicated, complicated, protracted and recurrent. Forecast. In the absence of complications, the prognosis is favorable, and in case of complications, it is serious. 18. DILATED (CONSTANT) CARDIOMYOPATHY Myocardial diseases of unknown etiology, manifested by cardiomegaly and heart failure, with the exclusion of damage to the heart valves, coronary and pulmonary vessels, arterial hypertension. Pathogenesis. A hypocirculatory hemodynamic state develops with a decrease in the stroke volume of the heart with increased filling of the heart with blood. Clinic. Extrasystole, ventricular tachycardia appear; atrial fibrillation, initially of a paroxysmal type, which quickly becomes permanent. Signs of circulatory decompensation. Systolic blood pressure decreases while maintaining diastolic blood pressure. The apex beat is weak, diffuse, the first sound is dull. At the apex of the heart, in the 4th intercostal space on the left near the sternum, a prolonged systolic murmur appears. Auscultatory signs increase with the progression of heart failure and cardiac dilatation and weaken as the condition improves. In the first asymptomatic period there are no complaints. The ejection fraction was reduced to 35%, the end-diastolic size of the left ventricle was 6,5 cm. In the II period of progressive myocardial damage, symptoms of chronic heart failure appear - NC stages I-II. Ejection fraction 35-25%, end diastolic size of the left ventricle 7-7,5 cm. In the III period of developed clinical manifestations, a clinic of total heart failure appears - NK IB-III, severe cardomegaly. Mortality is high from congestive heart failure, thromboembolic complications. In the IV period of stabilization, complete or significant regression of edema, venous congestion occurs with the progression of the actual signs of circulatory failure. In the fifth terminal period, severe degeneration of all internal organs occurs, ischemic damage to the liver, kidneys, discirculatory encephalopathy, loss of body weight, and recurrent thromboembolism is possible. Diagnostic study. Conducting a biochemical blood test (dysproteinemia, hypoalbuminemia in congestive heart failure). An ECG study reveals conduction rhythm disturbances. 24-hour Holter ECG monitoring and EchoCG are performed (dilatation of all cavities of the heart, mainly the left ventricle, decreased ejection fraction, and signs of heart failure are noted). Treatment. In the presence of tachysystolic atrial fibrillation and symptoms of left ventricular failure, cardiac glycosides (digoxin) are used; β-blockers are prescribed after stabilization of the condition with cardiac glycosides and diuretics. Potassium-sparing diuretics are used. ACE inhibitors have a beneficial effect on pre- and afterload with subsequent improvement in hemodynamics; nitrosorbide, cordarone, anticoagulant therapy, and blood ultrafiltration are used to reduce stagnation. Flow. Rapid progression (1-1,5 years), slow progression or recurrent. Forecast. Adverse. 19. HYPERTROPHIC CARDIOMYOPATHY Hypertrophy of the walls of the left ventricle (occasionally right) without expansion of the cavity, with increased systolic function and impaired diastolic function. Hypertrophy is more often asymmetric with a predominance of thickening of the interventricular septum, not associated with increased work of the heart. Pathogenesis. Asymmetric septal hypertrophy leads to dynamic, then fixed obstruction of the outflow tract from the left ventricle. The ability of the myocardium to relax is reduced. The diastolic function of the left ventricle worsens due to calcium overload of the cytoplasm of cardiomyocytes and a decrease in the elastic properties of the myocardium. Clinic. Shortness of breath, worsening with physical exertion, pain in the heart, muscle weakness, dizziness, fainting, palpitations, and attacks of loss of consciousness are noted. The disease can be asymptomatic or of the vegetodystonic type. During auscultation at the apex and at the Botkin point, a systolic murmur of great variability is heard. Diagnostic study. An ECG examination reveals signs of left ventricular hypertrophy; Atypical Q waves may appear - deep, narrow in leads II, III, aUR, V4, V5. Possible signs of WPW syndrome, repolarization disorders, ST segment reduction, T wave inversion. To detect ventricular tachycardia, atrial fibrillation, daily Holter ECG monitoring is performed. EchoCG study reveals changes in the thickness of the interventricular septum, which can reach 1,7-2 cm or more. Treatment. β-blockers are prescribed in large doses, which increase left ventricular filling, reduce the pressure gradient and have an antiarrhythmic effect. Calcium channel blockers are used. Verapamil has a negative inotropic effect on the myocardium, is prescribed 40-80 mg 3-4 times a day. Long-term treatment with this drug can lead to inhibition of automatism, deterioration of atrioventricular nodal conduction, and excessive negative inotropic action. You can not prescribe the drug with a large filling of the left ventricle, with orthopnea, nocturnal paroxysmal dyspnea. Nifedipine is inappropriate, as it increases the pressure gradient due to a pronounced vasodilating effect (syncope). Antiarrhythmic drugs are used. Cordarone is prescribed for ventricular arrhythmias: in the first week, 600-800 mg / day, then 150-400 mg daily with a two-day break every week. The effect of the drug comes in 1-2 weeks and persists for several months after withdrawal. Disopyramide is indicated for supraventricular and ventricular tachycardia. Physical activity is limited, with infections, timely antibiotic therapy is carried out. Cardiotonic agents, diuretics, nitrates, vasodilators are contraindicated in the treatment. Of the surgical methods of treatment, excision of a part of the interventricular septum and mitral valve replacement are used. Flow. Relatively favorable, progresses slowly. Forecast. Adverse. 20. RESTRICTIVE CARDIOMYOPATHY Restrictive cardiomyopathy is a decrease in myocardial compliance with limited filling of the left ventricle, a decrease in stroke volume and the development of heart failure. The group with these symptoms includes diseases with obliteration of the ventricular cavities, phenomena of atrioventricular regurgitation, and parietal thrombosis. Etiology. The disease is extremely rare and is often considered a complication of endomyocardial (eosinophilic) disease (Loeffler's fibroplastic myocarditis) and endocardial fibrosis, fibroelastosis. Pathological anatomy. The endocardium is primarily affected (except for endomyocardial fibrosis), and the myocardium is involved in later periods of the disease. Connective tissue develops, obliteration of the ventricular cavities and the development of parietal thrombosis occur, proliferation of endothelial cells leads to occlusion of small myocardial vessels. Clinic. Clinical manifestations are characterized by the appearance of complaints of shortness of breath, especially with physical exertion, chest pain, weight loss. In the initial periods, the boundaries of the heart are not changed, in the future there is an increase in the left or right ventricles (where fibrosis predominates), in the later periods there is an increase in toto. At the beginning, the tones are rhythmic, the third tone is heard, above the apex there is a systolic murmur. Symptoms of heart failure increase gradually. Diagnostic research. An ECG study determines changes characteristic of diffuse myocardial damage. X-ray examination reveals dilatation of the cavities of the heart, venous congestion in the lungs. Echocardiography reveals early rapid filling of the ventricles. A study of hemodynamic parameters is carried out, which establishes an increase in filling pressure in both ventricles, an increase in end-diastolic pressure in the left ventricle, and pressure in the pulmonary artery. When ventriculography is determined by increased contraction of the ventricles, smooth contours of the walls, a possible filling defect in the apex during obliteration. In life, the diagnosis can only be established by endomyocardial biopsy. Complications. Circulatory failure, thromboembolism, rhythm disturbances (less often than with hypertrophic cardiomyopathy). Differential diagnosis. Amyloidosis, hemochromatosis, sarcoidosis, scleroderma, idiopathic Abramov-Fiedler myocarditis (diagnosis is difficult even with autopsy). Treatment. In the early stages of the disease in the presence of eosinophilia, corticosteroids are used. Diuretics, vasodilators, anticoagulants (for the prevention of thromboembolism), calcium antagonists are used: they affect the diastolic function of the left ventricle. Surgical treatment is possible at the stage of fibrosis to remove the altered endocardium, prosthetics of the mitral and tricuspid valves. Flow. The course of the disease is slowly progressive. Forecast. With damage to the left ventricle - relatively favorable, with involvement in the process of the valvular apparatus - doubtful. 21. sinus tachycardia, sinus bradycardia, sinus arrhythmia, sinus node weakness syndrome 1. Sinus tachycardia Increased cardiac activity at rest more than 90 beats per minute with the correct rhythm. Etiology. It occurs due to an increase in the tone of the sympathetic nervous system. There are physiological and neurogenic. Tachycardia can be observed in diseases of the cardiovascular system, with drug and toxic effects, with acute and chronic infections and anemia. Clinic. Complaints are determined by the underlying disease. The I tone is strengthened, the II tone is more often weakened, the pendular rhythm and an embryocardia are possible. On the ECG, the heart rate is more than 90 beats per minute, the duration of the RR interval is less than 0,60 s, the rhythm is correct. Treatment. In the functional form, psychotropic and sedatives, tranquilizers, neuroleptics (meprobamate, diazepam), and β-blockers (atenolol, egilok in doses that do not reduce the number of heart contractions below 60 beats per minute) are used. 2. Sinus bradycardia Decrease in heart rate below 60, but not less than 40 per minute. Etiology. An increase in the tone of the vagus nerve, a decrease in the tone of the sympathetic nerve, a direct effect on the cells of the sinus node (hypoxemia, infection). Clinic. Manifested by palpitations, fainting. On the ECG, the RR interval is more than 1 s, the rhythm is sinus. Treatment. With organic bradycardia with a heart rate of less than 40 beats per minute and a tendency to faint, atropine is administered 0,5-1,0 mg intravenously every 3 hours (up to 2 mg) or 0,5-1,0 mg 3-4 times inside and others 3. Sinus arrhythmia Alternating periods of increased and decreased heart rate due to uneven generation of an impulse in the sinus node. Etiology. The reasons are fluctuations in the tone of the vagus during breathing, organic pathology of the heart (CHD, rheumatic heart disease, myocarditis, digitalis intoxication). Clinic. On the ECG, there is an irregular sinus rhythm with a difference between the longest and shortest P-P intervals of 0,16 si more. Treatment. It consists in the treatment of the underlying disease. 4. Sick sinus syndrome Paroxysms of supraventricular tachycardia (or atrial fibrillation) followed by a long period of severe sinus bradycardia. Etiology. Organic heart disease (acute period of myocardial infarction, atherosclerosis, myocarditis, cardiopathy, digitalis intoxication, antiarrhythmic drugs). Clinic. Possible sinus bradyarrhythmias, loss of individual sinus complexes with prolonged asystole and subsequent restoration of the rhythm. Depending on the duration of the periods of asystole, there may be dizziness, fainting, seizures of Morgani-Adams-Stokes. Treatment. With attacks of tachyarrhythmias and paroxysmal tachycardia, antiarrhythmic drugs are indicated: aymalin 50 mg intravenously or intramuscularly, procainamide intravenously or intramuscularly 5 ml of a 10% solution, isoptin intravenously 5-10 mg, inderal (obzidan) 5 mg intravenously carefully, strophanthin 0,5 .0,05 ml of XNUMX% solution, etc. 22. Rhythm of the atrioventricular junction, idioventricular rhythm, extrasystoles, paroxysmal tachycardia 1. Rhythm of the atrioventricular connection The pacemaker is the area of transition of the atrioventricular node into the bundle of His or the trunk of the bundle of His before it branches into branches. Etiology. Vagotonia (with a healthy heart), medicinal effects and metabolic disorders (digitis intoxication, quinidine, morphine, hyperkalemia, acidosis, hypoxia), organic heart disease (CHD, hypertension, heart defects, myocarditis, rheumatic heart disease, shock). Clinic. Bradycardia with the correct rhythm of 40-60 beats per minute, enhanced I tone, increased pulsation of the jugular veins. On the ECG, there is a negative P wave, an unchanged QRST complex. Treatment. The underlying disease is being treated. Atropine, isadrin, alupent are used. Antiarrhythmic drugs are contraindicated. For hyperkalemia and acidosis, drip administration of sodium bicarbonate and glucose with insulin is performed. In case of complete atrioventricular block, an artificial pacemaker is implanted. 2. Idioventricular rhythm The pacemaker of the heart becomes the center of the third order with a rare rate of contraction - 20-30 beats per minute. Etiology. Severe myocardial damage. On the ECG - altered QRST complexes (as in ventricular extrasystole), negative P waves. Treatment. The underlying disease is being treated. 3. Extrasystoles Contraction of the whole heart or any of its departments under the influence of a premature impulse from the cells of the conduction system of the atria and ventricles. Etiology. Re-entry of the sinus impulse (local blockade), increased automatism outside the sinus node. Treatment. Treatment of the underlying disease. A diet and regimen must be followed, and hydrotherapy must be used. Sedatives and antiarrhythmic treatment are prescribed (if necessary). If there is a threat of ventricular fibrillation, intravenous lidocaine or procainamide is indicated. 4. Paroxysmal tachycardia A sudden increase in heart rate as a result of impulses emanating from a focus located outside the sinus node. Etiology. Strong emotions, nervous tension, overwork, excessive use of nicotine, etc. thyrotoxicosis, reflex influences, WPW and CLC syndrome, myocardial diseases, hypertension, mitral stenosis, digitalis intoxication, hypokalemia. Treatment. Relief of supraventricular paroxysmal tachycardia: massage of the sinocarotid zone, use of the Valsalva maneuver (pressure on the eyeballs), 40 mg of propranolol orally, slow intravenous administration of 2-4 ml of 0,25% isoptin solution, in the absence of hypotension 5-10 ml of 10% - of a solution of novocainamide if there is no effect - defibrillation. Relief of an attack of ventricular paroxysmal tachycardia: electric pulse therapy, intravenous injection of lidocaine. For mild conditions, novocainamide 0,75 g orally and then 0,25 g every 3 hours or intravenously. 23. Atrial fibrillation, atrial flutter, ventricular fibrillation 1. Atrial fibrillation (atrial fibrillation) Complete prolapse of atrial systoles. Up to 350-600 pulses circulate in the myocardium. The rhythm of ventricular contractions is wrong. Etiology. Organic myocardial damage, thyrotoxicosis. Pathogenesis. The mechanism of excitation re-entry is micro reentry, stopping the sinus node. Clinic. General weakness, palpitations, shortness of breath. Auscultation determines the arrhythmia of tones, changes in the volume of tones; pulse deficit. There are no P waves on the ECG, ventricular complexes are irregular, the isoelectric line is wavy. Treatment. When stopping an attack, sedatives are used, propranolol inside; while maintaining the attack - 4-8 g of potassium chloride diluted in water, intravenous administration of 5,0-10,0 ml of a 10% solution of novocainamide. In the presence of heart failure in elderly patients, strophanthin is used. In persistent cases of atrial fibrillation, quinidine and electrical impulse therapy are used. For persistent atrial fibrillation, cardiac glycosides are prescribed. Defibrillation is performed for recently occurring (up to a year) atrial fibrillation. 2. Atrial flutter Accelerated, superficial, but the correct rhythm of atrial contraction with a frequency of 200-400 per minute. Etiology. Organic heart disease (valvular disease, ischemic heart disease, thyrotoxicosis, rheumatic heart disease, myocarditis, intoxication). Clinic. Forms: paroxysmal, constant. Treatment. It is carried out as in atrial fibrillation. 3. Ventricular fibrillation (ventricular fibrillation) Uncoordinated, asynchronous contractions of individual muscle fibers of the ventricles. Etiology. Organic heart diseases (CHD, acute myocardial infarction, etc., heart failure, postoperative period, hypothermia, WPW syndrome, intoxication, electrical injury. Pathogenesis. Weak, erratic contractions of the muscle fibers of the ventricles are noted, the aortic semilunar valves do not open. The stroke volume of the heart drops to zero, blood flow to the organs stops. Death occurs within 4-8 minutes. Clinic. Clinical manifestations are characterized by loss of consciousness, pallor, cold sweat. Arterial pressure drops to zero, heart sounds are not heard, there is no breathing, the pupils are dilated. The onset of death. Stage I - a reversible state for no more than 8 minutes (clinical death), Stage II - biological death. resuscitation activities. Carrying out artificial ventilation. In case of inefficiency, three-time defibrillation is performed. If there is no effect, 1 ml of a 0,1% solution of adrenaline is injected intravenously or 2 ml endotracheally, after the introduction, defibrillation is repeated. CPR must be carried out within 40 minutes. After resuscitation, lidocaine is administered intramuscularly every 2-3 hours for 6-8 days; β-blockers are prescribed over the next 8-18 months. 24. ARRYTHMIAS DUE TO IMPULSE CONDUCTION DISORDERS Conduction disturbances between the sinus node, atria and ventricles. Etiology. Organic heart disease, increased tone of the cholinergic system, intoxication (digitis, b-blockers). Treatment. With AV blockade of the XNUMXst degree, no treatment is required. With AV blockade of the degree of the proximal type, verapamil (Isoptin), potassium preparations, and cardiac glycosides are used. With complete AV blockade caused by digitalis, the drug is withdrawn. While maintaining the blockade, 0,5-1,0 ml of a 0,1% solution of atropine is injected intravenously, intramuscularly 5 ml of a 5% solution of unitiol 3-4 times a day. In case of sudden complete AV blockade, administration of quinidine, procainamide, ajmaline, and allapinine is indicated. With moderate sinoauricular blockade while maintaining the correct rhythm, treatment is not required. In severe cases, the use of atropine and sympathomimetes. With sick sinus syndrome and manifestations of Morgagni-Adams-Stokes syndrome, implantation of an artificial pacemaker is indicated. For ventricular arrhythmias, lidocaine, trimecaine, and diphenine are administered. Cardiac glycosides are completely contraindicated. With AV blockade and ventricular disorders, quinidine, novocainamide, b-blockers, cordarone, allapinin are used. WPW syndrome (Wolff-Parkinson-White) - shortening of atrioventricular conduction, the appearance of a delta wave (serration) on the ascending knee of the R wave and tachyarrhythmia attacks. Described in 1930, noted in apparently healthy young people with tachycardia attacks. Etiology. Etiological factors are a short atrioventricular node, the possible presence of two atrioventricular nodes, additional pathways for conducting impulses: Kent's bundle, Maheim's bundle, James's bundle. Clinic. Clinical manifestations may be absent. Attacks of supraventricular paroxysmal tachycardia are possible, and less commonly attacks of atrial flutter or atrial fibrillation. Sudden death and heart failure are extremely rare. The ECG shows a negative delta wave in leads II, III, aVF (must be differentiated from posterior diaphragmatic myocardial infarction). Treatment. With frequent attacks of tachycardia, preventive treatment is carried out. Syndrome LGL (Laun-Ganong-Levin) - shortening of PQ with an unchanged QRS complex, paroxysms of supraventricular tachycardia are possible. CLC (Clerk-Levy-Christerko) syndrome. Shortening of P-Q with an unchanged QRS complex, ventricular arrhythmias are possible. Parasystole - the presence of two pacemakers (sinus and ectopic), functioning independently; on the ECG: a constant distance from the previous normal ventricular complex to the ectopic one, a constant short interectopic interval, ventricular parasystole is more often noted. Ectopic activity of centers with exit blockade is a rare variant of parasystole, the ectopic pacemaker has a higher rate than the main one. 25. HEART FAILURE A pathological condition in which the cardiovascular system is unable to provide organs and tissues with the necessary amount of blood both at rest and during exercise. Etiology. Infectious-inflammatory and toxic lesions of the myocardium, myocardial blood supply disorders, metabolic disorders, overload of the heart with pressure, volume, heart defects such as valvular insufficiency, a combination of heart overload and myocardial damage, cardiac arrhythmia. Pathogenesis. In the initial period of heart failure, the functioning of cardiac and extracardiac compensation mechanisms is noted. Clinic. The initial stage of heart failure is characterized by the appearance of shortness of breath during exercise, dry cough at night, and nocturia. Auscultation is heard gallop rhythm, IV tone. Chronic left ventricular heart failure develops with aortic defects, mitral insufficiency, arterial hypertension, coronary artery disease, and diseases affecting the left ventricle. Shortness of breath, cyanosis, and cough appear. Congestive bronchitis with sputum production and hemoptysis develops. In the lungs there is hard breathing, in the lower parts there are moist small and medium-bubble rales, expansion of the heart to the left, tachycardia, accent of the second tone over the pulmonary artery. Chronic right ventricular heart failure develops with mitral defects, emphysema, pneumosclerosis, tricuspid valve insufficiency, congenital defects. There is stagnation of blood in the veins of the systemic circulation, shortness of breath, palpitations, swelling of the legs, pain and heaviness in the right hypochondrium, small diuresis. Expressed acrocyanosis, swelling of the cervical veins, cardiac impulse, epigastric pulsation, expansion of the heart to the right. Plesha's symptom and venous pulse, ascites, hydrothorax are noted. Diagnostic research. The colloid-osmotic state of the blood, the electrolyte balance of sodium, potassium, calcium, etc. The ECG reveals signs of overload of the left or right atrium, etc. EchoCG study determines an increase in cavities, a decrease in myocardial contractility. X-ray examination establishes the expansion of the cavities of the heart, central and peripheral venous congestion. Treatment. Table number 10 is assigned with the restriction of liquid and table salt. To improve myocardial contractile function, cardiac glycosides, β-adrenergic receptor stimulators, and ACE inhibitors are prescribed. Normalization of myocardial metabolism is carried out with potassium, ATP, B vitamins, amino acids, anabolic hormones. To improve peripheral circulation, caffeine, cordiamine, and peripheral vasodilators are used. The elimination of stagnation in the small circle is carried out by bloodletting, the use of fast-acting diuretics - uregit, mannitol. To increase the tone of the cardiovascular system, exercise therapy, massage, carbon dioxide and hydrogen sulfide baths are prescribed. Forecast. In stages I and IIA - relatively favorable, in stage IB - serious, in stage III - unfavorable. 26. PNEUMONIA (ETIOLOGY, PATHOGENESIS, CLASSIFICATION, CLINIC) An acute infectious and inflammatory process in the lungs involving all the structural elements of the lung tissue and obligatory damage to the alveoli of the lungs. Etiology. In all cases they are caused by gram-positive or gram-negative microflora. In immunodeficiency pneumonia, Pneumocystis carinii, Cytomegalovirus, Herpes simplex, and fungi are found. With aspiration pneumonia, anaerobic microorganisms are detected. Pathogenesis. In community-acquired pneumonia, damage to the endothelium of the tracheobronchial tree occurs with disruption of mucociliary clearance and the mucociliary barrier. The functioning of macrophages and the secretion of lysozyme and interferon are disrupted. With nosocomial pneumonia, the cough reflex is suppressed, the mucous membrane of the tracheobronchial tree is damaged during surgery and artificial ventilation, and there is also a sharp decrease in general and local immune defense against the background of immunosuppressive therapy. Classification. They are divided into community-acquired, or home, outpatient, nosocomial, or hospital, nosocomial, aspiration, in persons with severe immunity defects. The severity is: 1) mild: mild intoxication (consciousness is clear, fever up to 38 ° C, tachycardia up to 90 beats per minute, blood pressure is normal), shortness of breath is slight on exertion, not at rest, on the x-ray - the lesion is small; 2) moderate: moderately severe intoxication (clear consciousness, mild euphoria, sweating, weakness, fever up to 39 ° C, tachycardia up to 100 beats per minute, moderate decrease in blood pressure), shortness of breath at rest (number of breaths up to 30 per minute), on an x-ray - pronounced infiltration of lung tissue; 3) severe degree: severe intoxication (temperature up to 39-40 °C, adynamia, blackout, delirium, tachycardia more than 100 beats per minute, collapse), shortness of breath at rest (30-40 respiratory movements per minute), cyanosis, extensive infiltration on x-ray, complications of pneumonia are common. According to the prevalence of pneumonia, there are lobar, segmental, right-sided, left-sided. Clinic. Hot flash stage: acute onset: chills, headache, chest pain when breathing, fever, dry cough, later “rusty” sputum appears. Herpes labialis (nasalis), hyperemia of the cheek on the affected side, and swelling of the wings of the nose may appear. When breathing, the affected half of the chest lags behind the healthy one. Percussion - pulmonary sound with a tympanic tint. Auscultation - weakening of vesicular breathing, gentle initial crepitation - "indux" crepitation, pleural friction noise. In the thickening stage, a cough with purulent sputum, constant fever, shortness of breath, chest pain when breathing and coughing, mental agitation, Herpes, flushing of the cheeks, icterus of the skin and sclera appear. Voice tremors and bronchophony increase. A dull sound is detected by percussion. On auscultation, bronchial breathing and pleural friction noise are heard. In the resolution stage, a productive cough appears, a large amount of sputum, body temperature drops. Percussion is determined by dullness with a tympanic shade. Harsh breathing, rough crepitus - "redux" crepitus, sonorous moist rales are auscultated. 27. PNEUMONIA (DIAGNOSTICS, TREATMENT, PROGNOSIS, PREVENTION) Diagnostic research. A general blood test is performed (leukocytosis, increased ESR). A biochemical study of blood is determined by dysproteinemia. A bacterioscopy with Gram staining and culture of sputum obtained during deep coughing and determination of antigens by polymerase chain reaction are performed. The pleural fluid is examined (counting leukocytes with a leukocyte formula, determining pH, LDH activity, protein content, Gram smear, culture for aerobes, anaerobes, mycobacteria). Fibrobronchoscopy is also performed with a quantitative assessment of microbial contamination (to exclude pulmonary tuberculosis) and chest radiography. Treatment. Provides for active and early impact on the pathogen, the use of rational antibacterial therapy, anti-inflammatory treatment through the complex use of physiotherapeutic treatment and medications (NSAIDs), the elimination of toxemia, correction of dysfunction of the lungs and other systems (rehabilitation), pathogenetic and symptomatic therapy. Bronchodilators are used in combination with mucolytics to improve the drainage function of the lungs (ambroxol, mucodin, bromhexine, bronchicum, etc.); for bronchial obstruction - bronchodilators with an anticholinergic effect (Atrovent, Berodual). Patients are indicated for early therapeutic breathing exercises (if the temperature drops to low-grade and there are no hemodynamic disturbances), physiotherapeutic treatment (microwave field to the area of the pneumonic focus) in the absence of contraindications (abscess formation, hemoptysis, suspicion of a tumor or specific process, the presence of severe cardiac pathology). At the end of the course of antibacterial therapy, in the absence of contraindications from the gastrointestinal tract, NSAIDs are prescribed. Antibacterial therapy for non-severe pneumonia can be completed upon reaching a stable temperature normalization (within 3-4 days); the duration of treatment is usually 7-10 days. In severe pneumonia, a two-stage method of using antibiotics is used, the transition from parenteral to oral administration should be carried out as soon as possible, taking into account the clinical condition. The criteria for the sufficiency of antibiotic therapy are body temperature below 37,5 ° C, no intoxication, no respiratory failure, no purulent sputum, normalization of blood parameters: leukocytes below 10 l, neutrophils below 80%, young people below 6, no negative dynamics on the radiograph. Transition criteria (on average 2-3 days after the start of treatment): normalization of temperature (below 37,5 °C) with two consecutive measurements at an interval of 8 hours, reduction of shortness of breath, absence of impairment of consciousness, positive dynamics of other symptoms of the disease, absence of gastrointestinal absorption disorders , patient consent to oral treatment. Flow. Acute, protracted and chronic. Forecast. In the absence of complications - favorable, in the presence of complications it is determined by them. Prevention. Hardening of the body, smoking cessation, dispensary observation of those who have been ill. 28. CHRONIC BRONCHITIS A diffuse inflammatory-degenerative process in the bronchial mucosa and peribronchial tissue, manifested by a constant or periodic cough with sputum for at least 3 months a year for 2 years or more. Etiology. Causative factors: smoking, infection (viral or bacterial), toxic exposure, occupational hazards, deficiency of β-1-antitrypsin, household air pollution. Pathogenesis. Hyperplasia of goblet cells of the bronchial glands occurs, hypersecretion of mucus in the bronchi and changes in its properties, inflammatory edema and infiltration of the bronchial mucosa, disruption of bronchial patency and drainage function of the bronchi, imbalance between proteinase inhibitors (a-1-antitrypsin) and proteinases (neutrophil elastase). Clinic. With simple chronic bronchitis, cough, malaise, weakness, increased fatigue are noted, auscultatory: hard breathing, sometimes weakened. With mucopurulent chronic bronchitis, moist, sonorous fine bubbling rales may occur. In chronic obstructive bronchitis, there is an increase in cough, sputum, shortness of breath, diffuse cyanosis (lips, earlobes, acrocyanosis), rare deep breathing, barrel-shaped chest. Percussion displacement of the borders of the lungs down, their immobility, boxed sound. Auscultatory - uniform weakened breathing with prolonged expiration, scattered dry buzzing rales, disappearing after coughing. Diagnostic study. A general blood test is performed (leukocytosis, increased ESR in simple and mucopurulent bronchitis during exacerbations, hematocrit in obstructive bronchitis in men more than 52%, in women more than 47%). Immunological blood test (decreased activity of nonspecific and humoral components of the immune response, increased activity of the cellular component in obstructive bronchitis), sputum examination (macro- and microstudy - cytology, flora). The functional state of the lungs is examined (determination of volume and velocity indicators) - peak fluometry, spirography, and pneumotachometry are used. Computed tomography (morphological changes in the lungs, their location, size), ECG (exclusion of cardiac origin of symptoms, determination of hypertrophy of the right heart. Complications. Focal pneumonia, emphysema, respiratory failure, chronic cor pulmonale, secondary erythrocytosis, bronchiectasis. Treatment. In the acute phase, antibacterial therapy (in the presence of purulent sputum), M-anticholinergics, b2-agonists, methylxanthines, mucolytics, antihistamines, oxygen therapy, therapeutic bronchoscopy, physiotherapeutic procedures, physical therapy, treatment of complications. In the remission phase, bronchodilators (if indicated), mucolytics (used for symptoms of mucostasis), physiotherapy, spa treatment. Flow. Recurrent, chronic, progressive. Prevention. The following: timely treatment of acute bronchitis and respiratory diseases, early detection and treatment of the initial stages of chronic bronchitis, hardening of the body. 29. BRONCHIOECTATIC DISEASE Regional expansion of the bronchi with a predominant localization of the process in the lower parts of the lungs, manifested by chronic endobronchial suppuration. The disease is associated with genetic defects in the development of the bronchi observed in children and adults. Men get sick more often. Bronchiectasis does not include secondary bronchiectasis, in which damage to the lung tissue predominates due to an active inflammatory process. Etiology. Etiological factors include bronchopulmonary infections, aspiration of foreign bodies, bronchial stenosis with secretion retention and constant suppuration distal to the stenosis, bronchial malformations, congenital predisposition (Sievert-Kartagener syndrome). Pathogenesis. Bronchial patency is disrupted (formation of obstructive atelectasis), inflammation of the bronchi occurs, intrabronchial pressure increases, the elasticity and mechanical stability of the bronchi decreases, and obstruction of the small bronchi occurs (cystic fibrosis). Clinic. The main manifestations of the disease are: productive cough, mainly in the morning, with the release of a significant amount of mucopurulent or purulent sputum, hemoptysis. Sputum production depends on the position of the body - it increases in a state of orthopnea. Patients note intoxication, weight loss, increased body temperature, puffiness of the face, an earthy tint of diffuse cyanosis, and retraction of the affected side of the chest. Fingers in the shape of drumsticks, nails in the shape of watch glasses (a sign of hypoxia). During percussion, the mosaic nature of the percussion sound is determined (a low-specific sign). Auscultation reveals harsh breathing, pockets of persistent moist medium- and coarse-bubbling rales, and loud dry rales. Diagnostic study. A general blood test is performed, which reveals anemia, neutrophilic leukocytosis with a shift to the left, and an increase in ESR. A general urine test, a biochemical blood test (dysproteinemia: hypoproteinemia, albuminemia, hypergammaglobulinemia), and sputum examination (macro- and microscopic study of the flora: three-layered, many leukocytes) are also performed. During bronchoscopy, a lot of sputum is found in the lumen of the bronchi, hyperemia of the mucous membrane, and a continuous flow of sputum are noted. With bronchography - bronchiectasis of various shapes, with radiography - a decrease in the volume of the affected lung, a cellular pattern of the lungs. A functional study of the lungs is being carried out. Treatment. Patients are prescribed diet No. 15, active positional drainage according to B. E. Votchal. Antibacterial drugs are prescribed (parenterally and intrabronchially), repeated sanitary bronchoscopy, bronchodilator therapy, mucolytics, desensitizing agents, anabolic hormones, vitamins (groups B, C), with frequent exacerbations and the prevalence of bronchiectasis in no more than one lobe, surgical treatment (segmental resection) is indicated , lobectomy). Flow. Progressive, long-term remissions are possible. Forecast. With a limited lesion - favorable, and with a widespread process and the presence of complications - unfavorable. Prevention. Timely treatment of lung infections, smoking cessation, systematic positional drainage, treatment of complications. 30. LUNG ABSCESS Limited purulent inflammation of the lung tissue with destruction of its parenchyma and bronchi, their melting and the formation of a cavity. Etiology. Obstruction of the bronchi by foreign bodies, acute pneumonia, bronchiectasis, chest trauma, hematogenous embolization by infection. Pathogenesis. There is a penetration of the infectious agent into the lung tissue (bronchogenic, hematogenous, lymphogenous pathways, aspiration of foreign bodies), a violation of the drainage function of the bronchi. Classification According to the characteristics of the clinical course, the disease is divided: 1) by origin: acute lung abscess and chronic lung abscess; 2) by localization (segment, segments, right- or left-sided); 3) by complications. Clinic. In acute lung abscess (OAL), a period of organization is distinguished (up to 7 days before the opening of the cavity), which is characterized by an acute onset (dry hacking cough, chills), a change from chills to torrential sweat (hectic fever), mental disorders, puffiness of the face, flushing of the cheeks , lagging of the affected side of the chest during breathing, local thickening of percussion sound, hard breathing with a bronchial tinge, and a period after opening the cavity, characterized by a sudden discharge of purulent, fetid sputum with a full mouth, a drop in temperature, and a decrease in intoxication. Percussion over the affected area of the lung is determined by the appearance of tympanitis, with auscultation, amphoric breathing, moist medium and large bubbling sonorous rales. With chronic lung abscess (CHAL), patients have a cough with foul-smelling sputum, hemoptysis, chills, sweating, puffiness of the face, diffuse cyanosis, bad breath, fingers in the form of drumsticks, nails in the form of watch glasses (a sign of hypoxia), the overlying area amphoric breathing and moist, sonorous fine-bubble rales are heard. Diagnostic study. A general blood test is carried out, in which, during the organization period, neutrophilic leukocytosis with a sharp shift to the left, increased ESR is determined, in the period after the autopsy - normalization of indicators; with CAL - neutrophilic leukocytosis with a shift to the left, an increase in ESR. An immunological blood test is also carried out (lymphopenia, increased activity of the nonspecific and humoral components of the immune response), sputum examination (macro- and microstudy - cytology, flora, elastic fibers), X-ray examination (during the organization - massive darkening with unclear contours; after autopsy in bronchus - a cavity with thick, infiltrated walls and a horizontal level of liquid; with a breakthrough into the pleura - free liquid and gas in the pleural cavity). Flow. Acute and chronic. Treatment. Careful care for patients is required, high-quality nutrition with sufficient amounts of protein and vitamins (diet No. 15), infusions of nutritional mixtures, drug treatment, which includes antibacterial therapy, detoxification therapy, bronchospasmolytic therapy, positional drainage, endoscopic sanitation of the bronchi, the use of heparin (to prevent DIC syndrome), mucolytic and expectorant drugs. 31. GANGRENE OF THE LUNG Gangrene of the lung is a progressive necrosis and hypochorous (putrefactive) decay of the lung tissue, not prone to limitation. The disease is inherited by a recessive type, as a rule, it is not transmitted from parents to children. Etiology. The causative agents of the disease are non-clostridial anaerobes. Diseases such as chronic alcoholism, diabetes mellitus, and pneumonia in weakened patients predispose to the development of lung gangrene. The immediate causes may be: penetration of foreign bodies into the respiratory tract, lobar pneumonia, abscess or echinococcus in the lung; various diseases of the blood vessels. There are immunological and non-immunological forms of lung gangrene; there are also a number of options: atopic, infectious-allergic, dishormonal, autoimmune, neuropsychic, adrenergic imbalance, primary altered bronchial reactivity, cholinergic. Pathogenesis. Anaerobic bacteria penetrate into the lung tissue, activation of bacterial exotoxins and their direct effect on lung tissue, progressive lung tissue necrosis, vascular thrombosis in the affected area, impaired formation of granulation tissue. Clinic. The main manifestations of the disease are cough with foul-smelling sputum and fragments of lung tissue, hectic fever, chest pain, shortness of breath; percussion at the onset of the disease reveals expanding dullness; during the peak period - the appearance of areas of tympanitis due to the formation of cavities. On palpation, pain is determined over the affected area (Kiessling's symptom) and percussion (Sauerbruch syndrome) (involvement of the pleura in the process), palpation - first, an increase in vocal tremors, then a weakening. Auscultation is heard, first bronchial breathing, then a sharp weakening of breathing. Additional diagnostic study. A general blood test is performed, where neutrophilic leukocytosis is determined with a sharp shift to the left, increased ESR. A study of sputum is also carried out (during macro-examination, sputum forms 3 layers: the upper one is foamy, liquid; the middle one is serous; the lower one is fragments of decaying lung tissue; micro-examination is the study of flora, cytology), X-ray examination (massive infiltration without clear boundaries with the presence of multiple confluent cavities irregular shape). Differential diagnosis. Should be carried out with tuberculosis, lung cancer. Flow. The course of the disease is severe and progressive. Treatment. Antibacterial therapy is carried out (parenterally, intravenously), possibly injected into the pulmonary artery. They combine several types of antibacterial drugs. Detoxification therapy is carried out (reopolyglucin, hemodez, hemosorption, ultraviolet irradiation of autologous blood), bronchospasmolytic therapy, endoscopic sanitation of the bronchi with subsequent administration of antibiotics, enzymes, antiseptics, blood transfusion (in case of anemia development), heparin is used (to prevent disseminated intravascular coagulation syndrome). Prevention. Preventive measures include adequate treatment of acute pneumonia, adequate bronchial drainage, rehabilitation of chronic infection foci, smoking cessation. 32. THROMBOEMBOLISM OF THE PULMONARY ARTERY (PE) Blockage of the arterial bed of the lung by a thrombus formed in the venous system, right atrium, ventricle of the heart, or other material that has entered these areas. Etiology. Venous thrombus (in 85% of cases the source is in the inferior vena cava system, much less often in the right chambers of the heart and veins of the upper extremities) - drops of fat, tumor cells, air, parasites, foreign bodies. Risk factors include advanced age, atherosclerosis, the presence of malignant tumors, pregnancy, contraceptives, obesity, varicose veins. Pathogenesis. The triad of R. Virchow is characteristic: slowing down the speed of blood flow, increasing blood clotting, damage to the vascular wall. Classification. The disease is divided 1) downstream: acute, subacute, recurrent; 2) according to the affected area: small (up to 25% of the volume of the switched off channel), submassive (up to 26-50%), massive (up to 51-75%), lethal (more than 75%); 3) according to the severity of manifestations. Clinic. The main syndromes are: pulmonary-pleural (bronchospasm, shortness of breath, cough, hemoptysis, pleural friction noise, pleural effusion), cardiac (retrosternal pain, tachycardia, accent II tone, systolic and diastolic murmurs over the pulmonary artery, pericardial friction murmur, hypotension , swelling of the cervical veins, cyanosis), abdominal (pain in the right upper quadrant of the abdomen), cerebral (loss of consciousness, convulsions, paresis), renal (anuria). According to the significance and degree of manifestations, the symptoms are distributed in the following sequence: tachycardia, chest pain, shortness of breath, hemoptysis, fever, moist rales, cyanosis, cough, pleural friction noise, collapse. Diagnostic study. A sputum examination and a study of the blood coagulation system are carried out (moderate hypercoagulation, increased levels of platelet b-thromboglobulin and decreased antithrombin III). ECG: tachycardia, deviations of the atrial and ventricular vectors to the right, transient blockade of the right bundle branch. X-ray examination: expansion of the lung root, diffuse depletion of the pulmonary pattern. Perfusion scintigraphy is indicated (registration of radiation over the lungs after intravenous administration of a colloidal solution of protein labeled with technetium) - with PE, a decrease in radiation. Flow. Associated with the risk of death. Treatment. In acute PE at stage I, an urgent intravenous administration of 10-000 IU of heparin is performed, sedatives, analgesics are prescribed, and oxygen is given. At the II stage, streptokinase (15 IU intravenously drip), vasoactive drugs, antiacidotic therapy, heparin administration (000-250 IU 000 times a day under control of blood coagulation) are indicated. At the III stage, an embolectomy is performed - in the absence of the effect of the I and II stages of treatment and no later than 5000 hours from the onset of the disease. For recurrent pulmonary embolism, long-term use of indirect anticoagulants (6-12 months) is indicated. Prevention Timely treatment of the threatened contingent, reduction in the amount of animal fats and cholesterol in food. 33. CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) Chronic obstructive pulmonary disease is a heterogeneous group of pulmonary diseases that are combined by a disorder of the function of external respiration of the lungs according to the obstructive type. They are diagnosed at late stages, when progression becomes inevitable, despite the use of modern treatment programs. COPD includes chronic diseases of the respiratory system: chronic obstructive bronchitis (88-90%), severe bronchial asthma (8-10%), emphysema (1%). In the US and UK, the COPD group also includes cystic fibrosis, bronchitis obliterans, and bronchiectasis. With generalized obstruction, differential diagnosis is carried out. Pathogenesis, clinic, diagnosis and treatment of individual nosological forms of COPD are described independently. Management in an outpatient setting. Early identification of patients is necessary (for mild and moderate cases of the disease), early prescription of adequate basic therapy (for mild COPD, 3-week therapy with Atrovent is required with the possible addition of mucolytics, further prescription of bronchodilators according to indications (meteorological conditions, nature of work, bad habits), with Moderate and severe COPD requires long-term (constant) use of bronchodilators (Atrovent, Berodual 2 doses 3-4 times a day), if necessary, Saltos, Teopec, Theodur, etc. are added, for mucostasis - mucolytics; bronchodilators can be discontinued when stabilization of the subjective state and persistent stabilization of peak expiratory flow rates for 3 months). Monitoring is carried out for patients after ARVI or influenza with a long-lasting cough, non-productive, spastic in nature, not controlled by taking antitussive drugs (prescribing Atrovent for 3 weeks). Etiology. The reasons for the status may be resistance to sympathomimetics and other bronchodilators, rapidly developing total pulmonary obstruction, the development of hypoxia and hypercapnia. Clinic. There are 3 stages of flow. At stage 1, there is a discrepancy between distant noises and auscultatory data, tachycardia, a tendency to increase pressure, resistance to cardiac glycosides, accent and splitting of the II tone over the pulmonary artery, anxiety, tension, asthenia, pale cyanosis. In stage 2, respiratory failure, tachypnea, oligopnea increase, the sonority and number of dry rales decrease, their disappearance is possible, the formation of a "silent" lung, hypotension, decompensated respiratory acidosis and hypercapnia. In stage 3, there is pronounced diffuse cyanosis, loss of consciousness with the participation of all reflexes, "silent" lung syndrome, frequent and small pulse, sonorous heart sounds, hypotension, collapse, hypoxic coma is formed. Treatment. Treatment consists of avoiding b2-agonists, glucocorticoids (up to 1500 mg per day of prednisolone) are administered parenterally and orally, rehydration therapy (up to 3 liters of fluid per day), epidural anesthesia, artificial ventilation with bronchoalveolar therapeutic lavage. 34. BRONCHIAL ASTHMA (ETIOLOGY, PATHOGENESIS, CLASSIFICATION, CLINIC, DIAGNOSIS) A chronic inflammatory disease of the airways in which many cells and cellular elements play a role. Chronic inflammation causes a concomitant increase in airway hyperresponsiveness, leading to recurrent episodes of wheezing, shortness of breath, chest tightness, and coughing, especially at night or in the early morning. These episodes are usually associated with widespread but variable airflow obstruction. Etiology. The causes that cause the development of the disease are divided into internal factors (innate characteristics of the body) and external factors (modify the likelihood of developing the disease in predisposed people). Pathogenesis. A specific inflammatory process is formed in the bronchial wall in response to damaging risk factors (activated eosinophils, mast cells, macrophages, T-lymphocytes), bronchial obstruction develops, bronchial hyperreactivity increases. Airway obstruction has 4 forms: acute bronchoconstriction (due to spasm of smooth muscles), subacute (due to swelling of the mucous membrane of the respiratory tract), obstructive (due to the formation of mucous plugs), sclerotic (sclerosis of the bronchial wall with a long and severe course of the disease). Classification. Asthma can be: with a predominance of an allergic component, non-allergic, mixed. When making a diagnosis, the etiology, severity of the course, and complications are taken into account. Clinic. The period of precursors is characterized by a runny nose, sneezing, watery eyes, a feeling of sore throat, and a paroxysmal cough appears. In the extended period, patients take a forced position (orthopnea), there is expiratory dyspnea, distant dry wheezing, deep rare breathing, diffuse cyanosis, swelling of the cervical veins, auxiliary muscles are involved in the act of breathing, there is an expansion of the intercostal spaces. Percussion is determined by hard breathing, a lot of dry wheezing. Increasing tachycardia. During the period of resolution, a cough appears with difficult-to-discharge glassy viscous sputum, and distant wheezing disappears. Percussion is determined by the reduction of boxed sound. Auscultation - reduction of dry wheezing. Diagnostic research. A general blood test is performed, where leukocytosis, eosinophilia, and an increase in ESR are detected. The allergic status (presence of IgE) is determined, skin tests with allergens are performed. Sputum is examined (macroscopically - viscous, transparent; microscopically - eosinophils, Charcot-Leiden crystals and Kurshman spirals, neutrophils). A functional study of the lungs is carried out (a study of OVF1, FZhEL, PSV), samples with bronchodilators are put (a study of airway hyperreactivity). A non-invasive measurement of airway inflammation markers is carried out (sputum examination for the presence of eosinophils or metachromatic cells after inhalation of hypertonic saline or spontaneously isolated). NaECG: overload of the right ventricle. Flow. More often progressive, periods of exacerbations and remissions. 35. BRONCHIAL ASTHMA (TREATMENT, PREVENTION) Treatment. It is selected based on the severity of the course, the availability of anti-asthma drugs, the individual living conditions of the patient to ensure minimal severity of chronic symptoms, including nocturnal symptoms. Inhaled glucocorticoids: becotide, beclocort, pulmicort, ingocort, becladzhet. The route of administration is inhalation. Systemic glucocorticoids: prednisone, prednisolone, methylprednisolone. Route of administration: oral or parenteral. Cromones: sodium cromoglycate (Intal), sodium nedocromil (Tyled). They stabilize the membrane of mast cells and suppress the indirect release of IgE from them. Prescribed by inhalation, mainly for mild persistent bronchial asthma. Methylxanthines: theophylline, aminophylline, aminophylline, theodur, teopek, teoteolek, theotard, retophil. Used to control the course of bronchial asthma. Route of administration: oral. Long-acting inhaled b2-agonists: formoterol, salmeterol. The duration of action is more than 12 hours. Relax the smooth muscles of the bronchi, increase mucociliary clearance, reduce vascular permeability. Short-acting inhaled b2-agonists: fenoterol, pirbuterol, procaterol, salbutamol, terbutaline, berotek, asthmapent. The duration of action is from 4 to 6 hours. The route of administration is inhalation. Short-acting oral b2-agonists: salbutamol, terbutaline, bambuterol. They relax the smooth muscles of the bronchi, increase mucociliary clearance, reduce vascular permeability, and modulate the release of mediators from mast cells and basophils. Anti-leukotriene drugs: montelukast, pranlukast, zafirlukast - cysteinyl-leukotriene receptor antagonists, zileuton - 5-lipoxygenase inhibitor. Second generation antihistamines: (H1 blockers): acrivastine, astemizole, acelastine, cetirizine, ebastine, fexofenadine, ketotifen, loratadine, mizolastine, terfenadine. Suppress the development of allergic reactions. Route of administration: oral. Systemic nonsteroidal therapy: troleandomycin, methotrexate, cyclosporine, gold preparations. Include immunomodulators for unwanted effects of glucocorticoids to reduce the need for oral glucocorticoids. They are prescribed only under the supervision of a pulmonologist. The route of administration is oral. For a mild attack of suffocation, inhalation of short-acting b2-agonists (Berotec or salbutamol) up to 6 times within an hour, inhalation of anticholinergics (Atrovent, Troventol) simultaneously or independently, taking methylxanthines (aminophylline tablets) simultaneously or independently is indicated. Relief of moderate suffocation is carried out as therapy for a mild attack of suffocation by adding (optional): aminophylline 2,4% - 10,0 ml intravenously in a stream, ephedrine 5% - 0,5 ml subcutaneously, alupenta 1 ml intravenously in a stream . Corticosteroids are used orally or by infusion (if there is no effect). If there is no effect, stop administering b2-agonists. Forecast. In severe cases - disability. 36. PULMONARY EMPHYSEMA A condition characterized by an increase in the size of the air spaces located distal to the terminal or non-respiratory bronchioles due to expansion or destruction of their walls. Etiology. The cause of the disease can be chronic obstructive pulmonary disease, chronic pneumonia, pneumoconiosis, tuberculosis. Pathogenesis. There is a narrowing of the lumen of the bronchi, an increase in intra-alveolar pressure, thinning of the walls of the alveoli, a violation of their trophism, elasticity, development of alveolitis, destruction of the interalveolar septa. Classification. Emphysema has forms: interstitial, mediastinal, compensatory. Clinically, pulmonary emphysema is classified: 1) by origin: primary (idiopathic) - hereditary insufficiency of a-1-antripsin, b-2-macroglobulin, secondary (due to the development of chronic obstruction of the bronchial lumen); 2) by the nature of development: acute (due to sudden prolonged bronchial obstruction - after an attack of bronchial asthma), chronic (due to the presence of permanent bronchial obstruction); 3) by complications. Clinic. Primary pulmonary emphysema is manifested by shortness of breath (uncaused) of an expiratory nature, unproductive cough, and the appearance of an emphysematous (breathing) type of obstruction. With secondary emphysema, a pink complexion, dry cough is noted, with exacerbation of chronic bronchitis with mucopurulent or purulent sputum, expiratory shortness of breath. It develops gradually and begins to bother you in the 6th-7th decade of life. There is a barrel-shaped chest, retraction of the intercostal spaces when inhaling, participation of auxiliary muscles in breathing, a short neck, swelling of the jugular veins, and acrocyanosis. A bronchotic type of obstruction appears (“cyanotic edema”), patients lose weight, and often sleep sitting. On percussion, there is a boxy tint, the lower borders of the lungs are lowered by 1-2 ribs, their mobility is limited, the apexes of the lungs bulge above the clavicles. The pulmonary heart is formed according to the right ventricular type (in the terminal stages), liver enlargement. Diagnostic research. A general blood test is performed, where compensatory erythrocytosis, a moderate increase in ESR are noted. A functional study of the lungs is carried out - there is a decrease in the forced expiratory rate, a decrease in the Tiffno index, a decrease in the vital capacity of the lungs with an increase in the total and residual capacity, a decrease in the diffuse capacity of the lungs. Inhalation tests with bronchodilators are negative. The ECG shows right atrial hypertrophy (increased P and right ventricle (S)). X-ray examination - increased transparency of the lung fields, low standing of the diaphragm, dilated intercostal spaces. Treatment. If there is a bronchopulmonary infection, antibiotics are prescribed. Bronchodilators (M-anticholinergics, b2-agonists, methylxanthines), mucolytics, oxygen therapy, physiotherapeutic procedures, therapeutic exercises, spa treatment (in the absence of severe pulmonary heart failure) are indicated. Flow. Chronic, progressive. Forecast. Adverse. 37. LUNG CANCER Lung cancer is common. It mainly affects men aged 40-60 years. Etiology. The etiology is not known. Contribute to the occurrence of lung cancer: exposure to carcinogens (nickel, cobalt, iron), inhalation of dust in the mining industry, products of incomplete combustion of fuel in automobile engines, exposure to tobacco smoke, chronic inflammatory processes in the lungs, aggravated heredity, immunodeficiency states. Pathogenesis. Exophytic-endobronchial damage to the glandular epithelium of large bronchi occurs (1st, 2nd, less often 3rd order), then passes to the lung tissue (usually on the right, with localization in the upper lobes, less often in the lower and middle lobes), mediastinal organs , regional lymph nodes. The corresponding proportion of the lung decreases, and the mediastinal organs shift towards the lesion. A secondary inflammatory process develops in the affected area. Extrapulmonary metastasis with damage to the liver, bone marrow, and bone marrow. Clinic. Main manifestations: cough (associated with the development of reactive bronchitis, then pulmonary atelectasis, perifocal pneumonia, collapse of lung tissue), the nature of the cough is paroxysmal, whooping cough, initially dry, later with mucopurulent sputum, mixed with blood (clots, pulmonary hemorrhage). There is pain in the chest on the damaged side, the intensity of the pain increases as the tumor grows into the chest wall, the ribs and vertebrae are affected by metastases. Dyspnea increases gradually and is noted with the development of pulmonary atelectasis, massive effusion in the pleura, and compression of the mediastinal organs. There is an increase in body temperature (inflammatory process, cancer intoxication, development of complications). Weakness, sweating, fatigue, weight loss, and retraction of the chest wall on the affected side develop. Percussion dullness of sound over the lesion. Auscultatory weakened vesicular breathing, in the presence of pleural effusion - pleural friction rub. Diagnostic research. A general blood test is performed (anemia, neutrophilic leukocytosis with a shift to the left, an increase in ESR). An immunological blood test is carried out (an immunodeficiency state, a decrease in the activity of all parts of the immune response), a functional study of the lungs (a decrease in volume and speed indicators), and a sputum examination (cytology). X-ray examination: with central cancer of the upper lobe and middle lobe bronchi, darkening of the entire lobe or segment develops with a decrease in the volume of the lobe of the lung. With cancer of the main bronchus, its stenosis appears with a shift of the mediastinum to the diseased side. With peripheral lung cancer there is a dense rounded shadow with a diameter of 1-5 cm, more often in the upper lobes. Treatment. Early surgical treatment, radiation therapy, chemotherapy, symptomatic treatment of complications. Flow. Rapid progression. Forecast. Adverse. Prevention. Reducing dust, air pollution, combating occupational hazards, combating smoking, effective treatment of pneumonia. 38. EXOGENOUS ALLERGIC ALVEOLITIS A group of diseases caused by intense and prolonged inhalation of organic and inorganic dust antigens and characterized by allergic diffuse damage to the alveolar and interstitial structures of the lungs. General signs of the disease. The inflammatory process is localized in the alveoli and interstitium of the lungs, and not in the airways. Damaged areas consist of polynuclear and mononuclear infiltrates, sarcoid-like granulomas; in the later stages - the development of interstitial fibrosis. There is a development of III and IV types of allergic reactions. Etiology. Microorganisms (bacteria, fungi, protozoa) and their metabolic products (proteins, glyco- and lipoproteins, polysaccharides, enzymes, endotoxins), biologically active substances of animal and plant origin, low molecular weight compounds and medications. Pathogenesis. Type I pneumocytes are damaged, re-epithelialization of type II pneumocytes is impaired, and the activity of suppressor T-lymphocytes is reduced. Clinic. The acute stage develops 4-12 hours after contact with the allergen. Chills, fever, cough, shortness of breath, nausea, myalgia and arthralgia (flu-like syndrome) appear, crepitus and moist rales can be heard in the lungs (pneumonia-like syndrome), there may be a dry non-productive cough with expiratory shortness of breath and dry scattered wheezing (bronchitis syndrome), upon repeated contact with the allergen, symptoms may recur with a subacute (intermittent) course. In the chronic stage, a typical “Monday phenomenon”: acute manifestations are noted on the days after rest, disappear by the end of the working week (this form is diagnosed more often). Respiratory failure gradually progresses, asthenic syndrome, anorexia, weight loss with the formation of a chronic form appear, pulmonary hypertension and cor pulmonale are formed. Diagnostic research. A general blood test is performed (neutrophilia, increased ESR, eosinophilia), an immunological blood test (the activity of all parts of the immune response), skin tests with allergens, an inhalation provocative test with an antigen are performed. X-ray examination is being carried out. Differential diagnosis. In the acute stage with ARVI, influenza, acute pneumonia, acute bronchitis. In the chronic stage - with idiopathic fibrosing alveolitis, granulomatous processes in the lungs (tuberculosis, sarcoidosis, Wegener's granulomatosis). Treatment. In the acute phase, mandatory hospitalization. Glucocorticoid hormones are shown: prednisolone 40-60 mg/day for 1-3 days, followed by a decrease, with the ineffectiveness of hormone therapy, immunosuppressors, with fibrosis D-penicillamine (cuprenil). Extracorporeal methods are used: plasmapheresis, hemosorption. Flow. Prolonged, progressive. Forecast. Relatively favorable. Prevention. Primary prevention: development of technological processes of production, restriction of work in hazardous industries with bronchopulmonary diseases. Secondary prevention: dispensary observation. 39. FIBROSING ALVEOLITIS Fibrosing alveolitis is characterized by widespread fibrosis of the lungs below the level of the terminal bronchi (respiratory bronchioles and alveoli), leading to the development of an alveolar-capillary block and a sharp decrease in the diffusion capacity of the lungs, manifested by increasing pulmonary insufficiency. Etiology. The etiology of the disease remains unknown. Inheritance follows a dominant pattern. The disease is more common in men (ratio 1,9: 1), the most common age of patients: 40-70 years. Pathogenesis. Then the permeability of the air-hematic barrier increases, as a result of which interstitial edema and inflammation develop, exudate appears in the lumen of the alveoli and hyaline membranes form an irreversible stage of fibrosis, and progressive respiratory failure develops. Clinic. In the acute form, manifestations of an acute respiratory infection or pneumonia are characteristic, in the chronic form - progressive shortness of breath, unproductive or dry cough, fever to subfebrile (febrile), weakness, fatigue. The severity of shortness of breath and meager physical manifestations do not correspond to each other. Cyanosis, tachypnea, weight loss, change in the terminal phalanges of the fingers (drum sticks, watch glasses) are noted. Percussion is determined by the shortening of the lung sound, especially over the lower sections. Gentle crepitant rales, expressed in the basal regions, tachycardia, accent of the II tone over the pulmonary artery, in the later stages - signs of chronic cor pulmonale are auscultated. Additional diagnostic testing. A general blood test (moderate leukocytosis, leukopenia, increased ESR, signs of anemia), a biochemical blood test (dysproteinemia, hypergammaglobulinemia), an immunological blood test (increased immunoglobulins of classes C and M, the appearance of antinuclear antibodies), an X-ray examination (increased and deformed pulmonary pattern) are performed. , its looping, nodular focal shadows, possible decrease in the transparency of the lung tissue), functional examination of the lungs (the presence of restrictive nature of external respiration disorders), examination of blood gases (decreased diffusion capacity). Complications. Chronic cor pulmonale is the main complication of the disease. Differential diagnosis. Should be carried out with pulmonary insufficiency, pulmonary-cardiac insufficiency. Treatment. Corticosteroids are indicated (early use, long-term use), a combination of corticosteroids with immunosuppressants. It is possible to use afferent methods (hemosorption, plasmapheresis). During the period of remission, the use of aminoquinol drugs (delagil) is indicated. Flow. The course of the disease is relapsing, progressive, often chronic. Forecast. Unfavorable, average life expectancy 3-5 years. The main causes of death are severe respiratory failure, pulmonary hypertension, and lung cancer. 40. SARCOIDOSIS (BENE-BECK-SCHAUMANN DISEASE) Formation of non-caseating epithelial and giant cell granulomas with the greatest localization in the lung tissue. At the same time, the intrathoracic lymph nodes, liver, spleen, skin, eyes, nervous system, and heart can be affected. The disease is relatively rare, more common in men in young and middle age. Etiology. The cause of the disease is not clear. Pathogenesis. The immunological mechanism of development is inhibition of the T-cell immune response. Alveolar macrophages are activated and accumulate in the form of sarcoid granulomas. Classification. It has varieties: pulmonary sarcoidosis, lymph node sarcoidosis, pulmonary sarcoidosis with lymph node sarcoidosis. Clinic. Main syndromes: damage to lung tissue, dermatological, arthropathic, otthalmological. At stage I of the disease, weakness, general malaise, low-grade fever, sweating, pain in muscles and joints are noted, a dry cough appears, shortness of breath, swelling of the joints, and erythema nodosum appears on the skin of the extremities. There are no percussion changes. On auscultation, a small amount of dry and moist fine bubbling rales are heard. At the II stage of the disease, malaise, weakness, loss of appetite, weight loss, shortness of breath occurs already at rest. Percussion without changes. An increase in the number of dry and wet small bubbling rales, a pleural friction rub is auscultated. At stage III of the disease, the symptoms of stage II are accompanied by cough with mucopurulent sputum, hemoptysis, cyanosis, and shortness of breath at rest. Auscultatory heard a significant amount of scattered dry and moist rales. Diagnostic research. With a general blood test, there is a slight increase in ESR, lymphopenia, anemia. They conduct a biochemical blood test (dysproteinemia, an increase in a- and g-globulins, hypercalcemia), an immunological blood test (a decrease in the activity of all parts of the immune response, a decrease in tuberculin sensitivity), a study of the function of external respiration (at stage I - an obstructive type of respiratory impairment; with stage II - a mixed type of violation; at stage III - a restrictive type of violation), X-ray examination (with Stage I - bilateral increase in the size of the hilar intrathoracic lymph nodes, with Stage II - the appearance of multiple foci in the lungs, mainly in the middle and lower sections and the root zone, at stage III - pronounced fibrosis, large, confluent focal formations). Treatment. Patients are advised to eat a diet with plenty of protein and limit salt. Glucocorticoids are prescribed (for all forms and stages of the disease), in courses of 3-6 months or more, initial dose of 30-40 mg, end of treatment after clinical and radiological effect, aminoquinolones (Delagil), potassium preparations, anabolic steroids (non-bolic 5 mg per day, retabolil 50 mg once every 1-2 weeks intramuscularly). Flow. In stage I of the disease, spontaneous recovery is possible, in stage II - recurrent, cure is possible, in stage III - slow progression of the disease. Forecast. The prognosis is relatively favorable, mortality is from 2 to 5%. 41. CHRONIC PULMONARY HEART Hypertrophy and (or) dilatation of the right heart due to pulmonary arterial hypertension due to a respiratory disease. Etiology. Bronchopulmonary disorders - obstructive and restrictive processes: polycystic pulmonary disease, chronic bronchitis, bronchial asthma, pulmonary emphysema, diffuse pneumofibrosis, pulmonary granulomatosis. Vascular lesions - primary pulmonary arterial hypertension, arteritis, repeated pulmonary embolisms, lung resections, damage to the thoracodiaphragmatic apparatus. Lesions of the spine, chest, their deformation, pleural cords, obesity. Pathogenesis. Pathogenetic stages: precapillary hypertension in the pulmonary circulation, right ventricular hypertrophy, right ventricular heart failure, development of pulmonary arterial hypertension, increase in cardiac output due to increased catecholamines caused by hypoxia, increased blood viscosity due to erythrocytosis in response to chronic hypoxia, development of bronchopulmonary anastomoses, increased intraalveolar pressure in broncho-obstructive pulmonary diseases. Clinic. The main manifestations are the following: shortness of breath, cyanosis (appears with II and III degrees of respiratory failure), swelling of the jugular veins, epigastric pulsation, tachycardia, expansion of the boundaries of the heart, especially to the right, deafness of heart tones, emphasis of the II tone over the pulmonary artery, enlargement and tenderness of the liver , peripheral edema, small diuresis (in a decompensated state). Diagnostic research. A general blood test, a study of a general urinalysis (the appearance of protein, cylinders during decompensation), a biochemical blood test (dysproteinemia), and a functional study of the lungs are carried out. On the ECG - signs of cor pulmonale: high P waves in the II and III standard leads (P - pulmonale), rightogram, pronounced S wave in the I standard lead and left chest leads, the appearance of Q in the III lead. A study of hemodynamics is carried out (increased central venous pressure, slowing down the speed of blood flow, increasing the volume of circulating blood). On EchoCG: an increase in thickness in a compensated state and an increase in the cavity in a decompensated state of the right ventricle. An X-ray examination is also performed. Treatment. Treatment is aimed at treating the underlying disease. For infection of the bronchopulmonary apparatus, antibiotics are used, for bronchial obstruction - bronchodilators, for pulmonary embolism - anticoagulants, fibrinolytic drugs, for thoradiaphragmatic cor pulmonale - artificial ventilation. Peripheral vasodilators are used to reduce pulmonary arterial hypertension (nitrates, apressin, calcium channel blockers, beta-agonists). Oxygen therapy, bloodletting of 2-200 ml with infusion of low-viscosity solutions (reopolyglucin) to reduce erythrocytosis, and infusion of sodium bicarbonate solution to reduce acidosis are carried out. Flow. The course of the disease is chronic and progressive. Forecast. Adverse. 42. PLEURITIS Inflammatory process in the pleura, which develops a second time and is a reflection of an independent disease in the body (tumor, pneumonia, tuberculosis, pancreatitis, trauma, etc.). Etiology. Etiological factors: exacerbation of the tuberculosis process in the lungs or intrathoracic lymph nodes, non-specific inflammatory processes in the lungs, rheumatism, collagenoses, heart attacks, lung tumors, chest trauma, acute and chronic infectious diseases (dry pleurisy). Pathogenesis. There is an excessive accumulation of pleural fluid. Clinic. With dry pleurisy, there is pain in the affected half of the chest, which intensifies with breathing and coughing; In case of phrenic pleurisy, pain radiates to the upper half of the abdomen or along the phrenic nerve (to the neck). The pain is most severe in the initial period. Body temperature is normal or subfebrile. On auscultation: breathing is weakened, a pleural friction noise is heard. With exudative pleurisy, there is a high body temperature, severe stabbing pain in the chest, intensifying with a deep breath, a painful dry cough, sweating, lack of appetite, shortness of breath, cyanosis, lag of the normal half of the chest when breathing, smoothness of the intercostal spaces. On the diseased side, the formation of the Garland triangle occurs with stimpanitis (between the spine and the ascending line of dullness), on the healthy side - the Rauchfus-Grocco triangle with dullness of percussion sound. During auscultation, weakening of breathing is heard in the affected area, in the area of Garland's triangle - with a bronchial tint, pleural friction noise is heard at the onset of the disease and during resorption of the exudate. Additional diagnostic study. A general blood test is performed (anemia, leukocytosis, an increase in ESR), a study of the pleural fluid (protein above 3%, relative density above 1,018, positive Rivalt test, many neutrophils in the sediment, straw-yellow color - with exudates, with empyema - pus), x-ray examination: intense darkening with an oblique upper border, shift of the mediastinum to the healthy side - with exudates, limited mobility of the dome of the diaphragm, lowering the transparency of the sinus on the corresponding side. Treatment. With dry pleurisy, the underlying disease is treated. Analgesics (up to narcotic), non-steroidal anti-inflammatory drugs are introduced. For pleural effusions, the underlying disease is treated, a diet rich in protein, vitamins, and limited in salt and liquid is prescribed. Antibacterial drugs are administered (taking into account the sensitivity of the flora), detoxification therapy is carried out (plasma replacement solutions, vitamins B, C), pleural punctures are performed with the evacuation of pleural fluid. Desensitizing therapy is prescribed. Flow. Prolonged, acute, subacute, chronic. Forecast. Depends on the underlying disease and the nature of the effusion, more often recovery. Prevention. It is aimed at the prevention and timely treatment of diseases that can be complicated by inflammatory processes in the pleura, early recognition of the presence of pleural effusion, and its evacuation. 43. DIFFUSE GLOMERULONEFRITIS (ETIOLOGY, PATORENESIS, CLINIC OF ACUTE GLOMERULONEFRITIS) Immune-mediated inflammation with a predominant initial lesion of the glomeruli and involvement of all renal structures in the pathological process. It is divided into acute and chronic glomerulonephritis. True acute glomerulonephritis is only one that is proven by intravital morphological examination. In other cases, chronic glomerulonephritis develops, which has an acute onset. Etiology. Exogenous factors: bacteria (b-hemolytic streptococcus of group A (strains 12, 43, 49), white staphylococcus, bovine corynebacterium, enterococci, typhoid salmonella, treponema pallidum, diplococci), viruses (cytomegalovirus, herpes simplex viruses, hepatitis B, Epstein- Barra), fungi (Candida albicans), parasites (malarial plasmodium, schistosome, toxoplasma), drugs, poisons, foreign serum. Endogenous factors: nuclear, brush border antigen, thyroglobulin, immunoglobulins, tumor and embryonic antigens, carcinomatous antigen. Pathogenesis. There is a passive transfer of the immune complex into the glomerulus and its deposition. Antibodies that react with a structural antigen or with a trigger non-glomerular autologous or exogenous antigen circulate in the bloodstream. There is hyperfiltration, an increase in the transcapillary gradient - acceleration of sclerosis in the remaining glomeruli. Clinic. The main syndromes of acute glomerulonephritis are the following: urinary, edematous, hypertensive, nephrotic. Diseases can occur in the form: deployed (cyclic) and monosymptomatic (latent). The cyclic form never begins at the height of infection, no earlier than 14-25 days after the onset of infection. It is characterized by an obligatory cyclical course, it develops acutely, weakness, swelling (mainly of the face), headache, decreased diuresis, urine the color of meat slop, and lower back pain appear. Arterial hypertension develops (systolic blood pressure does not exceed 180 mm Hg, diastolic blood pressure - 120 mm Hg), tachycardia, and there may be signs of acute cardiac (left ventricular) failure (shortness of breath, cough, attacks of cardiac asthma). There is an expansion of the boundaries of relative cardiac dullness, systolic murmur at the apex, emphasis of the second tone on the aorta, sometimes a gallop rhythm, dry and moist rales in the lungs. Urinary syndrome is characterized by proteinuria, cylindruria, macro- and microhematuria. Proteinuria is associated with gross damage to the vascular wall of the glomerular capillaries, through which albumins, globulins, and fibrinogen are released. Hematuria is a constant symptom. There is a small number of leukocytes. Edema persists for 10-15 days, disappears by the end of the 3rd week, blood pressure decreases, polyuria develops, urinary syndrome persists for more than 2 months, hyposthenuria appears, slight proteinuria may persist for a long time (0,03-0,1 g/day), residual hematuria, leukocyturia disappears at the end of the first month. The latent form is characterized by a gradual onset, without subjective manifestations, headaches, slight shortness of breath or swelling in the legs are possible, the duration of the condition is up to 2-6 months or more, the presence of an isolated urinary syndrome. Acute nephritis that has not resolved within a year is considered chronic glomerulonephritis. 44. Diffuse glomerulonephritis (CHRONIC GLOMERULONEPHRITIS CLINIC) The main syndromes of chronic glomerulonephritis: urinary, hypertensive, edematous, hyperlipidemia, hypoproteinemia, anemic, chronic renal failure. The forms of the course are: latent, hypertensive, nephrotic, mixed, malignant (subacute), terminal. The latent form is more often detected by chance, during the clinical examination. Characterized by long-term preservation of working capacity without signs of disease (up to 10-20 years), the presence of isolated urinary syndrome, isohypostenuria, low specific gravity of urine, nocturia, possibly increased blood pressure, hypoproteinemia, hypercholesterolemia, increased ESR. For a long time, the leading and only symptom of the hypertensive form is arterial hypertension. Initially, hypertension is intermittent in nature, in the future - permanent. On examination, there is an apex beat visible to the eye, an expansion of the relative dullness of the heart to the left, an accent of the II tone over the aorta, a gallop rhythm, with the progression of heart failure, there are manifestations of stagnation in the pulmonary circulation, hemoptysis, attacks of cardiac asthma, rarely - pulmonary edema. The fundus of the eye: neuroretinitis is moderate, only narrowing of the arteries persists for a long time. In the nephrotic form, trophic changes appear: dry skin, a decrease in its elasticity, muscle hypotrophy, edema develops due to a decrease in oncotic pressure, initially minor in the morning under the eyes, on the ankles, then permanent with a transition to the trunk; hydrothorax, ascites, hydropericardium. There is a dissociation of protein-lipid ratios (hypoproteinemia, hypercholesterolemia), urinary syndrome may appear: hematuria, decreased filtration function, blood pressure does not increase. The mixed form is characterized by the severity of edema, urinary syndrome, arterial hypertension, as well as the progressive course and development of renal failure (within 2-5 years). The malignant (subacute form) is characterized by a rapid and persistent decrease in kidney function, increasing changes in the fundus. The terminal form refers to the stage of renal decompensation and is associated with insufficiency of nitrogen excretory function. Nephrotic and hypertensive syndromes are expressed, levels of urea, creatinine, indican are increased, glomerular filtration is reduced, and the filtration fraction increases. Left ventricular heart failure, chronic renal failure, anemia, uremic stomatitis, gastritis, colitis, bronchitis, polyserositis. Differential diagnosis: hypertension, left ventricular heart failure, diabetic glomerulosclerosis, liver cirrhosis, amyloidosis, congestive kidney. 45. DIFFUSE GLOMERULONEFRITIS (LABORATORY DIAGNOSTICS OF THE DISEASE) Diagnostic research. A complete blood count (neurophilic leukocytosis, increased ESR, anemia), a biochemical blood test (increased fibrinogen, C-reactive protein, LDH4-5 alkaline phosphatase), and a general urine test are performed. In acute glomerulonephritis, a decrease in the amount of urine to 400-700 ml / day is characteristic, anuria rarely occurs, protein - from 1 to 10 g / day, albuminuria decreases after 7-10 days, the amount of protein becomes less than 1 g / day, erythrocytes, single hyaline and granular casts, a slight increase in the number of leukocytes, an increase in the specific gravity of urine. In chronic glomerulonephritis, in the stage of renal compensation, there is an increase in the amount of urine, a persistent decrease in specific gravity (isohyposthenuria), and nocturia. In chronic glomerulonephritis in the stage of renal decompensation, there is a decrease in the amount of urine, an increase in protein, specific gravity, urea, creatinine, and indican in the blood. A Nechiporenko test is performed (determining the number of erythrocytes, leukocytes and casts in 1 ml of urine: normally erythrocytes - up to 1000, leukocytes - up to 2000, casts - up to 50, with glomerulonephritis erythrocytes predominate over leukocytes), Kakovsky-Addis test (determining the number of erythrocytes, leukocytes , cylinders in the daily volume of urine: normally erythrocytes - up to 1, leukocytes - up to 000, cylinders - up to 000, with glomerulonephritis, erythrocytes predominate over leukocytes), urine culture with quantitative assessment of bacteriuria (if detected in 2 ml of urine more than 000 bacteria). They also determine enzymes in urine and determine b000-microglobulin in urine (b100-MG) (assessment of the functional state of the kidneys). When the tubules are damaged, protein readsorption is disrupted, b000-MG excretion increases, no other proteins are detected, the glomeruli are not affected; with isolated damage to the glomeruli, the b1-MG content is within normal limits, and medium molecular proteins (albumin) increase. A Zimnitsky test is performed to assess the ability of the kidneys to concentrate and dilute urine: under normal water and nutritional regimes, 8 portions of urine are collected separately, its quantity and relative density are determined; assess daytime (from 8 a.m. to 8 p.m.) and nighttime (from 8 p.m. to 8 a.m.) diuresis, dynamics of quantity, relative density of individual portions, and nocturia. In the Folgard concentration test (with dry diet), daily diuresis decreases to 300-500 ml, the specific gravity of urine increases, reaching 4-8 in 1028-1035 hours, not lower than 1025. Reberg-Tareev test: glomerular filtration rate for creatinine - 80-160 ml / min, tubular reabsorption - 98-99%, with glomerulonephritis, the indicators decrease; in acute glomerulonephritis, the changes are transient; in chronic glomerulonephritis, they are persistent. An immunological blood test is carried out, in case of acute glomerulonephritis and with exacerbation of chronic glomerulonephritis, the level of total complement and the 3rd fraction decreases, the number of circulating immune complexes, immunoglobulins of all classes increases, the titer of antistreptolysin O increases. 46. Diffuse glomerulonephritis (treatment, prognosis, prevention) They also conduct an ECG study (signs of left ventricular hypertrophy), an examination of the fundus (exudation, retinal edema, changes in the papillae of the optic nerve that appear with the development of chronic renal failure). Treatment. Patients are prescribed a diet and regimen: with sufficient kidney function, protein restriction (within 1 g/kg body weight), with the development of arterial hypertension, salt restriction, with edema - salt and water, restrictions during the period of severe inflammatory process. Glucocorticoids are prescribed (immunosuppressive, anti-inflammatory and desensitizing effects) - initial dose of 60 mg/day for 3 weeks, then reduced by 5 mg for 4 days to 40 mg, then by 2,5 mg for 2-3 days, maintenance therapy with persistent urinary syndrome. Cytostatics are administered (with a long process, the presence of a hypertensive syndrome, initial signs of renal failure, with the ineffectiveness of hormone therapy): azathioprine (daily dose of 150 mg), cyclophosphamide (daily dose of 200 mg) to suppress final immune responses; delagin, rezoquin, chloroquine. Anticoagulants and antiplatelet agents are also indicated - heparin 20 thousand units per day for 5 days, then 5 thousand units daily for up to 3-4 weeks, chimes up to 300 mg per day orally on an empty stomach for 6-8 months; for severe renal bleeding, aprotinin (an anti-fibrinolytic drug), non-steroidal anti-inflammatory drugs (metindole) 100-150 mg per day for 1-2 months or more for acute glomerulonephritis with the presence of nephrotic syndrome. Calcium channel blockers, angiotensin-converting enzyme inhibitors (as pathogenetic therapy), and reduction of proteinuria are prescribed. Symptomatic therapy is carried out: antihypertensive, diuretic drugs, calcium salts, cardiac glycosides, desensitizing agents, large doses of vitamin C are prescribed. In case of uncomplicated AGN, in the first days, complete exclusion of salt, fluid restriction, ascorbic acid, calcium gluconate, if necessary, correction electrolyte disorders. With a persistent course of arterial hypertension, it is necessary to connect pathogenetic, antihypertensive, diuretic therapy. Programmed hemodialysis is carried out (in the absence of the effect of treatment, with an increase in renal failure), plasmapheresis. Flow. In acute glomerulonephritis, there is usually a complete recovery or recovery with persistent proteinuria. In chronic glomerulonephritis, depending on the form, the course is progressive, with the development of chronic renal failure. Forecast. In acute glomerulonephritis, the prognosis is favorable (mortality rate is 2%), in chronic glomerulonephritis, it is favorable in the latent form and unfavorable in other forms. Prevention. Primary prevention - rehabilitation of foci of infection, their adequate treatment, only appropriate vaccination. Secondary prevention - dispensary observation, treatment of complications and exacerbations, rational employment. 47. CHRONIC PYELONEPHRITIS Inflammatory process involving the renal pelvis, calyces and renal parenchyma and predominantly affecting the interstitial tissue. Etiology. The old focus of the inflammatory process in the urinary tract, cystitis, pyelitis. The disease can also be the result of untreated acute pyelonephritis. Pathogenesis. The infection leads to disruption of urodynamics and stagnation of urine in the pelvis. Pyelovenous or pyelo-papillary refluxes, impaired lymphatic drainage, stasis, and hemodynamic changes develop. An inflammatory reaction develops. Clinic. It is detected many years after suffering inflammation of the urogenital area. Women get sick more often. The process can be one- or two-sided. It is characterized by low-symptomatic manifestations, it is possible to establish the disease by chance in the study of urine, an increase in blood pressure. The main symptoms: fatigue, headaches, epigastric pain, subfebrile condition, development of cystitis, dysuria, temperature rises only during exacerbation, chilling; unexplained fevers. Pain in the lumbar region is dull, constant, aggravated by bimanual palpation. Anemia develops even before kidney failure. Arterial hypertension is associated with renal ischemia, for a long time patients are subjectively well tolerated. Polyuria, pollakiuria, nocturia develop. Diagnostic study. A general blood test is performed (neutrophilic leukocytosis with a shift to the left, an increase in ESR during exacerbation, anemia), a general urine test (reduced specific gravity, moderate proteinuria, slight cylindruria, microhematuria, severe pyuria - there are many leukocytes, they predominate over red blood cells). With Kakovsky-Addis and Nechiporenko tests, an increase in the number of leukocytes is noted. In case of latent progression, a prednisolone or pyrogenal test is performed. Chronocystoscopy, excretory urography, ultrasound examination (expansion and deformation of the pelvis, calyces are noted, the structure of the parenchyma, echogenicity changes) and x-ray examination (visible expansion of the pelvis, necks, changes in the structure of the calyces, asymmetry of the lesion is characteristic even with a bilateral process). Treatment. Nitropreparations are used: furagin or furadonin 0,1 g 3 times a day, nitroxoline (5-NOC) 0,1 g 4 times a day, nalidixic acid (non-vigramon, blacks) 0,5-1 g 4 times a day 2 -3 weeks, fast-acting sulfonamides (etazol, urosulfan) 4-6 g per day, prolonged action (biseptol-480) 1-2 g per day up to 2 weeks, sulfalene 0,25 g 1 time per day for a long time, broad-spectrum antibiotics (with the ineffectiveness of nitrofurans and sulfonamides, with exacerbations). The course should be short but adequate. Recommend the use of 1,5-2 liters of liquid during the day in the form of water, fruit and vegetable juices, herbal medicine for 2-3 weeks, spa treatment. Flow. Long-term, with periods of exacerbations and remissions. Forecast. Favorable for uncomplicated forms, unfavorable for complications. Prevention. Timely treatment of acute pyelonephritis, treatment of coprostasis, chronic colitis, cholecystitis, sanitation of the oral cavity, proper nutrition with plenty of vitamins, preventive therapy with herbal preparations. 48. CHRONIC RENAL INSUFFICIENCY Gradually emerging and steadily progressive impairment of kidney function, leading to uremic intoxication. Etiology. Chronic glomerulonephritis, chronic pyelonephritis, diabetic glomerulonephritis, amyloidosis, polycystic kidney disease, kidney stones, adenoma, prostate cancer. Pathogenesis. Pathogenetic mechanisms of the disease: lack of parenchyma regeneration, inevitable structural changes in the parenchyma, reduction in the number of functioning nephrons, their atrophy and shrinkage, disruption of excretory, blood purification and homeostatic functions, retention of nitrogenous metabolic products in the blood: urea, uric acid, ammonia, amino acids, creatinine, guanidine, phosphate retention, increased plasma and extracellular fluid potassium levels, hypocalcemia. Clinic. In the subclinical form, an increase in the volume of fluid you drink (up to 3 liters per day), nocturia (up to 3 times per night), dryness, skin laxity, peeling, daytime sleepiness, weakness, fatigue, tinnitus, hearing loss. In the clinical form, signs of pulmonary heart failure, severe anemia, changes in the liver, gastrointestinal tract without dysfunction. In the terminal form: apathy, puffy face, dry skin, painful itching, muscle weakness, muscle twitching, large cramps, deep noisy breathing, chest pain, development of secondary pneumonia, moist rales, in the terminal stage - uremic pulmonary edema. Uremic pericarditis, hypertensive cardiovascular syndrome, uremic vasculitis, visceritis, and hypothermia develop. Anorexia, aversion to food, nausea, vomiting, heaviness, fullness in the epigastrium after eating, and thirst appear. Anemia, toxic leukocytosis with a neutrophil shift to the left, thrombocytopenia, and blood clotting disorders develop. Bone damage occurs, changes in the skeleton, secondary gout, change from polyuria to oligo- and anuria, urinary syndrome is slightly expressed. Diagnostic research. Conduct a study of blood serum creatinine, nitrogenous metabolic products, the state of electrolyte and mineral metabolism, acid-base state, ultrasound of the kidneys, ECG study. Treatment. A diet is shown to prevent the breakdown of one's own protein. Hyperkalemia is being eliminated: the introduction of large amounts of glucose, hyponatremia: intravenous administration of a 10% sodium chloride solution, hypernatremia: the administration of natridiuretics (10% calcium gluconate solution), tachystin (0,125 mg), acidosis: diet, soda enemas, intravenous administration alkaline solutions, alkalosis: ammonium or 200 ml of a 2% potassium chloride solution, anemia: testosterone 300 mg per week for 3-6 months; iron supplements only when they are deficient. Carry out hemodialysis, peritoneal dialysis. Antihypertensive diuretics are used. Forecast. The prognosis is determined by the phase of renal failure, the rate of its development. Prevention. Active treatment of major diseases, systematic planned secondary prevention of chronic renal failure, clinical examination. 49. Systemic lupus erythematosus Chronic polysyndromic disease, predominantly of young women and girls predisposed to it. Classification (according to V. A. Nasonova). When making a diagnosis, it is necessary to separate: 1) according to the form of the course: acute, subacute, chronic, with a continuously relapsing course (malignant); 2) according to the degree of activity (I - minimal, II - moderate, III - maximum); 3) by stages: I - initial, II - generalized, III - terminal. Clinic. In an acute course, an acute onset, the development of polysyndromicity over the next 3-6 months (lupus nephritis or CNS damage). In the subacute course, the onset is gradual, arthralgia and nonspecific skin lesions are pronounced. The flow is characterized by undulation. In the chronic course, relapses of individual syndromes are observed for a long time, the development of polysyndromicity at the 5-10th year, the development of deforming polyarthritis at the 10-15th year. Lupus crises are manifestations of the activity of the lupus process. Characterized by pronounced clinical polysymptomatics, changes in laboratory parameters, general trophic disorders. Criteria for diagnosis: rash in the zygomatic region ("butterfly"), discoid rash, photosensitivity, ulcers in the oral cavity - painless or painless, arthritis without destruction of cartilage, two or more peripheral joints, serositis (pleurisy, pericarditis), kidney damage ( persistent proteinuria, 0,5 g / day or more), neurological disorders (convulsions), hematological disorders, immune disorders (the appearance of antinuclear antibodies with an increase in their titer). If four or more signs are present, the diagnosis is considered reliable. Diagnostic study. A general blood test is carried out (anemia, hemoglobin less than 100 g/l, normo- or hypochromic leukopenia, thrombocytopenia, increased ESR during exacerbations), a biochemical blood test (dysproteinemia, hypoalbuminemia, increased a2-globulins in the acute period of the disease, g-globulins to chronic). An immunological blood test is required (LE cells, antibodies to DNA, to native DNA, ribonucleoprotein, and other nuclear substances). A general urine test (specific gravity, protein, formed elements, epithelium, salts) and a skin biopsy are performed. Treatment. Glucocorticoids are prescribed (prednisolone 50-60 mg followed by a decrease by 2,5-5 mg per week - for many years), immunosuppressants (azathioprine 100-150 mg, 6-mercaptopurine 150-200 mg, leukeran 10-15 mg ) - several months, then a maintenance dose of 50-100 mg for many months. It is possible to use pulse therapy: 1000 mg of methylprednisolone 3 days in a row or 3 times every other day in 100 ml of isotonic sodium chloride solution or 500 mg 2 times with the addition of 5000 units of heparin and suprastin; addition to conventional hormone therapy. 4-aminoquinoline drugs (chloroquine, delagil, plaquenil) are used for several years, non-steroidal anti-inflammatory drugs (butadione, indomethacin, etc.) for several years, anticoagulants for several months, antiplatelet agents for several months, plasmapheresis, hemosorption - up to 5-6 sessions. Forecast. The prognosis of the disease is unfavorable. 50. SYSTEMIC SCLERODERMA Chronic polysyndromic connective tissue disease occurs in young and middle-aged women. Classification. When refining the forecast, the classification of N. G. Guseva (1988) is used: 1) downstream; 2) according to the stage of the disease; 3) according to the degree of activity (see Table 1). Table 1 Determination of process activity in systemic scleroderma
Clinic. The main syndromes are vascular (Raynaud's syndrome), trophic disorders (rat bite symptom, ulcerative lesions), cutaneous (mask-like appearance of the face, skin thickening), articular-muscular (arthralgia in large joints, polyarthritis, fibrosing myositis, muscle weakness), visceral (lesions heart - non-coronary sclerosis, myocarditis, mitral disease, pericarditis, lungs - pneumosclerosis, digestive tract - dysphagia, gastritis, enteritis; kidney - chronic nephritis, acute scleroderma nephropathy, nervous system - polyradiculoneuritis, meningoencephalitis), asthenovegetative (weight loss, weakness, increased fatigue , unstable fever). In the chronic course, Raynaud's syndrome progresses. Over time, changes appear in the nail phalanges, thickening of the skin, periarticular tissues, the formation of contractures, osteolysis, and slowly progressive changes in internal organs. In subacute course, there is a dense swelling of the skin, recurrent polyarthritis, myositis, damage to internal organs. In an acute course, a rapidly progressive variant of the course is fibrinous and visceral lesions already in the first year of the disease, the formation of a scleroderma kidney. Diagnostic research. The examination algorithm corresponds to diagnostic tactics in connective tissue diseases. Criteria for diagnosis are skin changes in the form of dense edema, induration and atrophy, Raynaud's syndrome, osteolysis, soft tissue calcification, joint-muscular syndrome with the development of contractures, basal pneumonitis, macrofocal cardiosclerosis, damage to the digestive tract, esophagus, true scleroderma kidney, hyperpigmentation skin, trophic disorders, immune disorders, the appearance of antinuclear antibodies with an increase in their titer. If four or more signs are present, the diagnosis is considered reliable. Treatment. Hormones, immunosuppressants, 4-aminoquinoline drugs, non-steroidal anti-inflammatory drugs, anticoagulants, antiplatelet agents are used - as in other connective tissue diseases, anabolic hormones for cachexia. Physiotherapy is used. Forecast. In chronic course, the prognosis is relatively favorable, with stabilization, in acute and subacute course - unfavorable. 51. NODULAR PERIARTERITIS Systemic necrotizing vasculitis of arteries of medium and small caliber with the formation of vascular aneurysms and secondary damage to organs and systems. Clinic. The main syndromes of the disease are asthenovegetative (weight loss, wave-like fever with high temperatures that do not decrease under the influence of antibiotics, weakness, adynamia), cardiac (coronary insufficiency syndrome, possible heart attacks), hypertensive (arterial hypertension), pulmonary (pneumonitis, asthmatic syndrome), abdominal (abdominal pain, dyspepsia, bleeding), hepatolienal (liver enlargement is more common), nephrotic (nephritis, nephrosclerosis with typical clinical manifestations), neurological (polyneuritis), trophic changes (subcutaneous nodules), articular (polyarthralgia), Wegener's syndrome (triad : rhinitis, sinusitis with subsequent ulceration of the bones and cartilage of the nose; pulmonary vasculitis; kidney damage with the development of failure) (Table 2). Course options: acute, subacute, chronically recurrent. Diagnostic criteria are kidney damage with arterial hypertension, typical abdominal syndrome combined with dyspeptic disorders, pneumonitis or bronchial asthma with high eosinophilia, cardiac syndrome in the form of coronaritis, polyneuritis. Three out of five criteria are required for diagnosis. Diagnostic research. Examination algorithm as in systemic connective tissue diseases. Table 2 Clinical and morphological features
Treatment. Hormone therapy is carried out, a combination of glucocorticoids with cyclophosphamide and azathioprine - up to several years. Physiotherapy procedures are contraindicated. Symptomatic treatment is carried out. Forecast. Adverse. 52. RHEUMATOID ARTHRITIS Chronic systemic disease of the connective tissue with a progressive lesion of predominantly peripheral (synovial) joints according to the type of erosive-destructive polyarthritis. Classification: 1) according to clinical characteristics: poly-, oligo-, monoarthritis, the presence of visceritis, combination with other rheumatic diseases; 2) by the presence of rheumatoid factor: seropositive, seronegative; 3) according to the degree of activity: minimal I, moderate II, maximum III, remission; 4) according to the x-ray stage: I - osteoporosis, II - narrowing of the joint spaces, III - erosion, IV - ankylosis; 5) by functional insufficiency: I degree - professional ability is preserved, II degree - is lost, III degree - the ability to self-service is lost. Clinic. The main syndromes are articular (damage mainly to small joints of the hands and feet, ulceration of the cartilage surface of the joints, deformation, ankylosis, morning stiffness syndrome), cardiac (myocarditis, endocarditis with the formation of shallow heart disease, pericarditis), pulmonary (adhesive pleurisy, fibrosing pneumonitis) , renal (chronic glomerulonephritis, amyloidosis), trophic disorders (rheumatoid nodules in the periarticular tissues of the affected joints), vascular (digital arteritis in the area of the nail phalanges), asthenovegetative (fever, weight loss), anemic (secondary iron deficiency anemia). Main clinical forms: articular (80% of cases), benign, articular-visceral, Felty's syndrome (1% of cases) - pancytopenia, enlargement of the spleen and peripheral lymph nodes, malignant, rapidly progressive form, Sjögren's syndrome (involvement of the parenchyma of the salivary and lacrimal glands with subsequent atrophy). The basis of diagnosis are major and minor criteria. In the presence of large criteria, the diagnosis is considered reliable, less than seven criteria - probable. If all criteria are met, a diagnosis of rheumatoid arthritis can be made. Diagnostic research. The examination algorithm corresponds to that adopted for systemic connective tissue diseases. Treatment. Non-steroidal anti-inflammatory drugs are prescribed, with preference given to long-acting drugs. Hormone therapy (corticosteroids) is carried out, if non-steroidal anti-inflammatory drugs are ineffective and the process remains active - 15-20 mg with a slow decrease and the addition of non-steroidal anti-inflammatory drugs in increasing doses). Basic therapy is carried out with gold preparations (cryzanol 2 ml intramuscularly once a week for 1-7 months), aminoquinoline preparations: rezoquin, plaquenil. Plasmapheresis and hemosorption are performed. Flow. With the articular form - slowly progressive with gradual deformation of the joints (10-15 years), with the articular-visceral - rapidly progressive (2-3 years). Forecast. With the articular form - favorable, with the articular-visceral - unfavorable. Prevention. Long-term use of basic drugs, non-steroidal anti-inflammatory drugs. 53. ALLERGY Allergy - the appearance of increased sensitivity of the body to the allergen in response to repeated contact with it. Allergens are antigens that cause allergic reactions. Almost all high- and low-molecular compounds of organic and inorganic nature (antigens and haptens) can acquire the properties of allergens under certain conditions. Allergens are divided into: 1) household; 2) fungal; 3) animal origin; 4) medicinal; 5) food; 6) microbial; 7) vegetable; 8) simple chemicals. The initial penetration of the allergen into the body usually does not manifest itself in any way. a period of sensitization begins, during which the immune system prepares a response to repeated penetration of the allergen and produces antibodies. The intensity of an allergic reaction depends on the nature of the allergen, the exposure dose, the way the antigen enters, the genotype of the individual, and the state of the immune system. Manifestations of allergenicity depend on environmental factors - air temperature, humidity, wind speed. The rate of development of allergic reactions. Early allergic reactions (urticaria and anaphylactic shock) develop within 30 minutes after repeated administration of the drug. Delayed allergic reactions (urticaria, itching, bronzospasm, laryngeal edema) develop 2-72 hours after repeated use of the drug. Late allergic reactions develop no earlier than 72 hours after repeated administration of the drug. Allergic status is associated with a system of histocompatibility antigens: 1) hay fever with HLA-A1, B8; 2) atopic dermatitis with HLA-Bw35; 3) combinations of atopic dermatitis with rhinitis with HLA-Bw40; 4) combinations of atopic dermatitis with bronchial asthma with HLA-B12; 5) atopic eczema with HLA-A1 and HLA-B8 (simultaneously); 6) exogenous allergic alveolitis with HLA-Bw40; 7) genetically determined hyperproduction of IgE with HLA-Dw2. This form is inherited in an autosomal recessive manner and manifests itself during the 1st year of life. Patterns of the immune response to allergen exposure There are 3 stages of the immune response: Stage I - immunological: providing T-lymphocytes with an allergen by macrophages in combination with MHC proteins of class I or II, differentiation of CD4T helpers; increase in antibody titer, interaction of the allergen with antibodies; Stage II - pathochemical: the release of allergy mediators by various cellular elements - histamine, serotonin, kinins, leukotrienes, prostaglandins, chemotaxis factor, activated complement fractions; Stage III - pathophysiological: the development of clinical manifestations of allergic reactions. 54. DRUG DISEASE Drug disease is associated with the production of antibodies or the appearance of T-lymphocytes specific for the drug or its metabolites. Causes of development include repeated use of intolerable drugs. Ways of formation There are 5 types of drug allergic reactions based on the classification of F. Gell and R. Coombs (1964): 1) anaphylactic: sensitization of the body is associated with hyperproduction of cytophilic IgE, which is quickly fixed by the Fc fragment on tissue basophils - mast cells, and to a lesser extent on eosinophils and other cells; this is accompanied by a low concentration of IgE in plasma; 2) cytotoxic: sensitization is characterized by the production of antibodies against antigens that are direct or secondary components of cell membranes; antibodies are IgJ, less often - IgM; 3) immunocomplex: occurs when pathogenic circulating immune complexes (CIC) appear in the plasma; 4) cellular (delayed-type hypersensitivity): occurs on allergens that are part of large molecules, which are then phagocytosed by macrophages, without damaging antigenic determinants; 5) immunological stimulation: is a variant of the type 2 reaction, develops when antibodies to cell receptors appear. Clinical manifestations. Allergic reactions of immediate type. Caused by many drugs, most often penicillins, develop within 30 minutes after drug administration. Urticaria, Quincke's edema, bronchospasm, anaphylactic shock appear. Rarely, with the introduction of penicillins, Stevens-Johnson syndrome, Lyell's syndrome, interstitial nephritis, systemic vasculitis, hemolytic anemia, neutropenia, neuritis can develop. Cytotoxic allergic reactions. With this form, hematological disorders develop: autoimmune hemolytic anemia, thrombocytopenia, agranulocytosis. The kidneys are affected: with interstitial nephritis caused by methicillin, antibodies appear to the basement membrane of the renal tubules. Immune complex allergic reactions. Most often caused by penicillins, heterologous serums. Symptoms of serum sickness usually appear 1-3 weeks after administration of the serum. Urticaria, maculopapular rash, fever, arthralgia (large joints) develop, lymph nodes may enlarge, glomerulonephritis, peripheral neuropathy, systemic vasculitis, acute inflammatory demyelinating polyradiculoneutropathy may occur. It is possible to develop drug-induced lupus syndrome, vasculitis with symptoms of fever, hemorrhagic rash, often on the legs, with damage to the kidneys and lungs. Allergic reactions of the delayed type. These include allergic contact dermatitis (after topical use of drugs), acute pneumonitis, interstitial pneumonitis, encephalomyelitis, interstitial nephritis, drug-induced hepatitis, and vasculitis. Acute and interstitial pneumonitis is characterized by fever, shortness of breath, cough, eosinophilia, limited or extensive opacities in the lungs, pleural effusion, and respiratory failure. 55. DRUG DISEASE (DIAGNOSIS, COMPLICATION, TREATMENT) In a diagnostic study, skin tests are used: 1) in case of allergic reactions of immediate type: intradermal injection of an antigen is manifested by hyperemia and a blister at the injection site due to degranulation of mast cells and the release of inflammatory mediators; 2) in delayed-type allergic reactions, skin tests have no diagnostic value. Application tests reveal sensitization to drugs for topical use only. The level of specific IgE is determined with the production of a radioallergosorbent test or a histamine release reaction by mast cells. Immunological determination of specific IgJ and IgM to drugs, fixed in tissues or circulating immune complexes (CIC) is performed. To identify sensitized T-lymphocytes, the reaction of lymphocyte blast transformation (RBTL) is performed or cytokine production is evaluated. This method is more sensitive than RBTL. Provocative tests allow you to establish a connection between the use of the drug and the occurrence of an allergic reaction. Due to the high risk of developing severe allergic reactions, samples are used very rarely, only in a hospital. Complications. Allergy to drug metabolites, pseudo-allergic reactions. Differential diagnosis. Should be carried out with the primary side effect of the drug, which develops when using drugs in therapeutic doses and is associated with their direct effect on target organs. It is necessary to exclude the secondary side effect of the drug as a complication of drug treatment that is not associated with the direct effect of drugs on target organs. It is necessary to exclude: 1) idiosyncrasy, a qualitatively altered response to the drug, due to non-immune mechanisms; 2) drug intolerance - the appearance of side effects when prescribing drugs in low doses; 3) toxic manifestations that develop with an overdose of the drug; 4) systemic lupus erythematosus; 5) vasculitis; 6) dermatitis, skin diseases. Treatment. First of all, the drug that caused the allergic reaction is canceled. With an allergic reaction of type I, epinephrine, H1-blockers are prescribed, with allergic reactions of types II, III and IV - corticosteroids. Flow. depending on the type of allergic reaction. Recovery is complete. Forecast. With an allergic reaction of type I in case of untimely resuscitation, the prognosis is unfavorable. With allergic reactions II, III and IV types - favorable. Prevention. It is necessary to conduct a mandatory collection of an allergic history, to exclude drugs that often cause allergies. 56. TREATMENT OF ANAPHILACTIC SHOCK In anaphylactic shock, it is necessary to quickly assess the patency of the airways, indicators of external respiration and hemodynamics. The patient should be laid on his back with raised legs. At a stop of breath and blood circulation immediately start cardiopulmonary resuscitation. A tourniquet is applied above the injection site, every 10 minutes it is loosened for 1-2 minutes. A solution of adrenaline 1: 1000 is injected subcutaneously into the shoulder or thigh: for adults - 0,3-0,5 ml, for children - 0,01 ml / kg. The injection site of the injected allergenic drug (with the exception of the head, neck, hands and feet) is chipped with 0,1-0,3 ml of adrenaline solution 1: 1000. In case of arterial hypotension, 1 ml of adrenaline solution 1: 1000 is diluted in 10 ml of saline, the resulting solution 1:10 is given intravenously over 000-5 minutes. After that, if necessary, an infusion of adrenaline 10: 1 can be carried out. For this, 1000 ml of adrenaline 1: 1 is diluted in 1000 ml of a 250% glucose solution. The initial rate of administration is 50 μg / min, in the absence of side effects, the rate increases to 1 μg / min. To prevent the resumption of symptoms of an anaphylactic reaction, H1-blockers are prescribed: diphenhydramine - 1-2 mg / kg intravenously (for 5-10 minutes), intramuscularly or orally. A single dose should not exceed 100 mg. Then the drug is taken at 25-50 mg orally every 6 hours for 2 days. Additionally, H2-blockers of histamine receptors can be prescribed: cimetidine is used in a dose of 300 mg (for children 5-10 mg/kg) intravenously slowly, intramuscularly or orally every 6-8 hours, ranitidine in a dose of 50 mg intravenously slowly or intramuscularly every 6-8 hours h or 150 mg orally every 12 hours (children 2-4 mg/kg). If arterial hypotension and breathing problems persist, the patient is transferred to the intensive care unit, where the following medication measures are carried out: 1) intravenous fluid infusion through a catheter with a maximum diameter: 5% glucose solution in 0,45% sodium chloride solution - 2000-3000 ml / m2 per day. Within 1 hour, 500-2000 ml of liquid is injected, for children - up to 30 ml / kg .; 2) for bronchospasm, b2-adrenergic stimulants are used: 0,5-1,0 ml of 0,5% salbutamol solution; if bronchospasm persists, aminophylline 4-6 mg/kg is administered intravenously over 15-20 minutes; 3) if there is no effect from the treatment, adrenergic stimulants are prescribed: norepinephrine intravenously, 4-8 mg of norepinephrine is dissolved in 1000 ml of a 5% glucose solution in water or saline, the maximum rate of administration should not exceed 2 ml/min if the patient is taking glucagon , additionally β-blockers are prescribed 5-15 mcg/min intravenously; 4) instead of norepinephrine, dopamine may be prescribed, more often in patients with heart failure: 200 mg of dopamine is dissolved in 500 ml of a 5% glucose solution, administered intravenously at a rate of 0,3-1,2 mg / kg per hour; 5) with a pronounced edema of the upper respiratory tract, tracheal intubation or tracheostomy is indicated; 6) corticosteroids are prescribed in the early stages: hydrocortisone is administered at a dose of 7-10 mg/kg intravenously, then 5 mg/kg intravenously every 6 hours, the duration of treatment is no more than 2-3 days; 7) after stabilization of the condition, the administration of liquid and medication continues for up to several days (depending on the severity of the condition). Author: Myshkina A.K.
▪ Age-related psychology. Crib
Artificial leather for touch emulation
15.04.2024 Petgugu Global cat litter
15.04.2024 The attractiveness of caring men
14.04.2024
▪ The fog is killing the trees ▪ Microhybrid boom expected by 2017 ▪ 10-storey house built in a day ▪ LT5522 - signal frequency transfer mixer
▪ section of the site Your stories. Article selection ▪ article There was a case near Poltava. Popular expression ▪ What tree trunk is the largest in circumference? Detailed answer ▪ windsurfer article. Personal transport ▪ article Aniline mordants for bone. Simple recipes and tips ▪ article Line hold prefix. Encyclopedia of radio electronics and electrical engineering
Home page | Library | Articles | Website map | Site Reviews
www.diagram.com.ua |



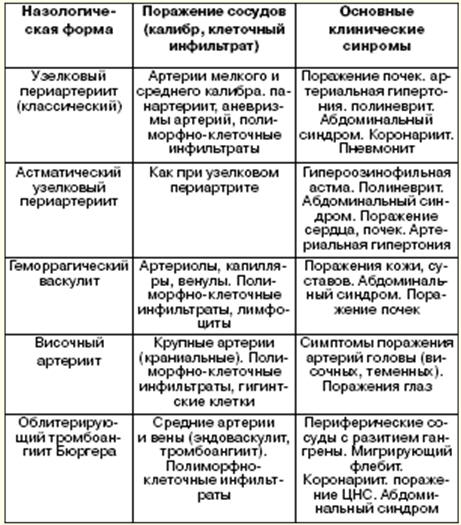
 See other articles Section
See other articles Section 