|
|






 Arabic
Arabic Bengali
Bengali Chinese
Chinese English
English French
French German
German Hebrew
Hebrew Hindi
Hindi Italian
Italian Japanese
Japanese Korean
Korean Malay
Malay Polish
Polish Portuguese
Portuguese Spanish
Spanish Turkish
Turkish Ukrainian
Ukrainian Vietnamese
Vietnamese|
Lecture notes, cheat sheets
Hospital therapy. Diseases of the cardiovascular system. Infectious endocaditis (lecture notes)
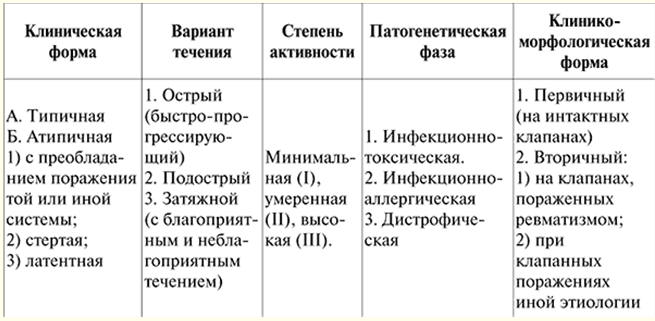
Directory / Lecture notes, cheat sheets Table of contents (expand) LECTURE No. 5. Diseases of the cardiovascular system. Infective endocaditis Infective endocarditis (IE) - a disease consisting in a polyposis-ulcerative lesion of the valvular apparatus of the heart (often with the development of valvular insufficiency) or parietal endocardium (less often, the endothelium of the aorta or the nearest large artery is affected). The disease is caused by various pathogenic microorganisms and is accompanied by a systemic lesion of the internal organs (kidneys, liver, spleen) against the background of an altered reactivity of the organism. Until now, in various printed publications, the previously used terms "bacterial endocarditis", "protracted septic endocarditis" can be found to refer to this pathological process. However, it is the term "infective endocarditis" that replaced them that better reflects the cause of the disease caused by a wide variety of microorganisms - bacterial agents, rickettsiae, viruses and fungi. The number of patients with IE is increasing worldwide. This is due to the presence of so-called risk groups (patients with atherosclerotic, rheumatic, traumatic valve injuries, heart or valve defects, ventricular septal defect, aortic coarctation) as a result of the fact that infection occurs more easily on a pathologically altered valve or endocardium. Etiology. The pathogenic causative agents of the disease are most often the coccal group of microorganisms - streptococci (viridans streptococcus was previously isolated in 90% of cases), staphylococci (golden, white), enterococcus, pneumococcus. In recent years, due to the widespread use of antibiotics, the range of microbial pathogens has changed. The disease can be caused by gram-negative flora (Escherichia coli, Pseudomonas aeruginosa, Proteus, Klebsiella); evidence has emerged of the important role of pathogenic fungi, Sarcinus, Brucella and viruses. Diseases caused by these pathogens are more severe, especially endocarditis caused by a fungal infection (usually occurs due to irrational use of antibiotics). However, in some patients the true causative agent of the disease is not detected (negative blood culture rate 20-50%). Often, infection occurs at the site of a prosthetic valve - the so-called prosthetic IE, which develops mainly within 2 months after heart valve replacement surgery. In this case, the causative agent of the disease most often has a streptococcal nature. Thus, the sources of infection and bacteremia in IE are very different (surgeries in the oral cavity, operations and diagnostic procedures in the urogenital area, surgical intervention on the cardiovascular system (including valve replacement), prolonged stay of the catheter in a vein, frequent intravenous infusions and endoscopic research methods, chronic hemodialysis (arteriovenous shunt), intravenous drug administration). There are so-called primary IE, which developed on intact valves, as well as IE against the background of congenital and acquired changes in the heart and its valvular apparatus - secondary endocarditis. These changes make it possible to distinguish patients into separate risk groups: heart defects (congenital and acquired), mitral valve prolapse, arteriovenous aneurysms, post-infarction aneurysms, shunts, condition after surgery on the heart and large vessels. Pathogenesis. The mechanism of development of IE is complex and insufficiently studied, however, the main points in the development of the disease can be identified. If there is a focus of infection in the body under the influence of altered humoral and local (cellular) immunity with a perversion of immunological reactions, various endogenous and exogenous factors, bacteremia develops. From the blood, microorganisms enter the heart valves, creating a secondary focus of infection there. The fixation and reproduction of microorganisms on the endocardium is facilitated by a number of factors: a previous change in the tissue and surface of the valve, the presence of thrombotic masses on it, arising under the influence of the direct damaging effect of the blood stream when its intracardiac circulation changes in conditions of existing heart disease. At the same time, various blood cells (platelets, etc.) “glue” to the site of traumatic injury, forming cell growths resembling icicles hanging from the valve. These vegetations become available for infection that has entered the vascular bed. Deformation of the valves due to the occurrence of a large pressure gradient, the narrowness of the hole and changes in blood flow velocity also contributes to the introduction of infectious agents into the endocardium with the formation of an infectious focus. When a previously intact valve is damaged, changes occur that disrupt the normal properties of individual sections of this valve (swelling appears), exudative or proliferative processes ("interstitial valvulitis" - preclinical phase). In the development of the disease, stage III can be distinguished. Stage I (infectious-toxic) proceeds with varying degrees of severity of intoxication. There is a growth of bacteria, the destruction of valves, leading to the development of heart disease; at the same stage, a generalization of the process often occurs due to the hematogenous spread of infection - pieces of cusps or colonies of microorganisms can separate from the valve, the cusps can rupture. The detachment of pieces of valve microbial vegetation contributes to the introduction of infected emboli into various parts of the vascular bed and exacerbates septic manifestations. Pieces of the valve or microbial vegetations circulate through the body with blood flow, when they enter the brain, they cause cerebral infarctions, which are accompanied by paralysis, paresis and various other neurological disorders. The valve, which has undergone destruction, cannot perform its function, and soon there is lightning-fast developing heart failure. Stage II - immuno-inflammatory, in which microorganisms fixed on the valves cause prolonged autosensitization and hyperergic damage to the organs and tissues of the body (immune generalization of the process). During this period, immune complexes circulate in the blood and are fixed in tissues (heart, kidneys, liver, blood vessels). Immune and autoimmune disorders cause the development of vasculitis and visceritis (immunocomplex nephritis, myocarditis, hepatitis, capillaritis, etc.). Stage III - dystrophic - occurs with the progression of the pathological process: the functions of a number of organs are disturbed, heart and kidney failure occurs, further aggravating the course of the disease. Classification. Currently, the classification and nomenclature of IE are used, reflecting the clinical form, course variant, degree of activity, pathogenetic phase and clinical and morphological form of the disease (see Table 6). Table 6 Classification of IE
A distinction is also made between active and inactive (healed) IE. There is also a surgical classification, in which they distinguish: 1) the lesion is limited to the valve leaflets; 2) the lesion extends beyond the valve. Acute IE (rapidly progressive, develops over 8-10 weeks) is rare, usually in individuals who have not previously had heart disease, and is clinically manifested by a picture of general sepsis. With modern methods of treatment, it is possible to translate it into subacute. Subacute IE (most common) lasts 3-4 months, with adequate drug therapy, remission may occur. However, relapses of the disease are possible. Protracted IE lasts for many months with periods of exacerbation and remission, it is characterized by mild clinical manifestations, minor laboratory parameters and general disturbances. The disease usually responds well to treatment. With an unfavorable course, severe complications arise, and patients die from progressive heart failure, increasing septic intoxication. clinical picture. Depending on the causative agent of the infection, IE can occur suddenly and develop rapidly (Staphylococcus aureus, enterococci) or have a latent onset (viridans streptococcus). Manifestations of IE are presented in the form of syndromes. 1) Syndrome of inflammatory changes and septicemia (fever, chills, hemorrhagic rashes, changes in acute phase blood parameters: leukocytosis with a shift to the left, an increase in ESR, the appearance of C-reactive protein, an increase in fibrinogen, α2-globulins. 2) Syndrome of general intoxication of the body (weakness, sweating, headaches, myalgia and arthralgia, loss of appetite, pallor of the skin with an icteric tint). 3) Syndrome of valve damage (formation of heart disease). 4) Syndrome of "laboratory" immune disorders (the presence of immune complexes circulating in the blood or fixed in the kidneys, myocardium, blood vessels; hypergammaglobulinemia; the appearance of rheumatoid factor; detection of anti-tissue antibodies). 5) Syndrome of thromboembolic complications (focal nephritis, myocardial infarction, spleen, intestines, thromboembolism in the brain, vessels of the lower extremities, etc.). 6) Syndrome of generalization of lesions (diffuse glomerulonephritis, myocarditis, hepatitis, vasculitis, etc.). The severity of these syndromes is different. It depends on the nature of the course of IE, stage, type of pathogen. For example, staphylococcal IE is characterized by high activity of the process, severe symptoms of general intoxication, and the development of purulent complications. Fungal endocarditis is usually accompanied by embolic occlusion of large arteries, especially of the lower extremities. A typical picture of the disease is characteristic of IE caused by streptococcus viridans. The onset of the disease is often associated with an acute infection or exacerbation of a chronic infection, as well as with a number of medical manipulations. Especially characteristic is the combination of an increase in body temperature of varying degrees (from prolonged fever to subfebrile condition or normal temperature) with chills and sweating. The patient presents simultaneous complaints due to the presence of an infectious process and intoxication, as well as thromboembolic complications of heart damage. Patients may have a history of episodes of long-term antibiotic treatment (this occurs when IE recurs in previously treated patients). Diagnostics. Of greatest importance for making a correct diagnosis is the detection of damage to the heart valves by changes in the auscultatory pattern of pre-existing heart defects; the appearance of “additional” noise. Characteristic lesions of the skin and mucous membranes are revealed: café au lait skin color, hemorrhages, positive Hecht's (pinch) and Konchalovsky-Rumpel-Leede (tourniquet) symptoms, as well as Osler's nodes - painful hyperemic dense nodules on the palmar surface and fingertips , Lukin-Libman sign (Lukin spots) - hemorrhage on the transitional fold of the conjunctiva. Splenomegaly is often observed in IE. Significant weight loss (sometimes 15-20 kg) is very typical. In rare cases, pericarditis develops (a faint pleural friction noise caused by fibrinous deposits on the pericardium). Physical examination may reveal increased blood pressure, indicating the development of diffuse glomerulonephritis. Sometimes signs of dysfunction of the central nervous system (paresis, hyperkinesis, pathological reflexes, etc.) as a result of embolism of cerebral vessels are determined. In this case, the most common diagnostic error is the assessment of a particular syndrome as a manifestation of an independent disease (for example, with pronounced signs of liver damage, hepatitis is diagnosed, etc.). However, the diagnosis of IE is based primarily on the early detection of the causative agent of the disease. For this, the following laboratory and instrumental studies are used. 1) Obtaining a positive blood culture is the most important diagnostic sign of IE. Analysis is also necessary to select the most effective antibiotic in this case. At least 2-3 of them are required to confirm the diagnosis. Of great importance are the technique of blood sampling and culture, the time of inoculation (preferably at the height of fever), the use of enriched media. 2) Carrying out NBT (nitrobluttetrazolium test) - diagnosticum of systemic bacterial infections, which allows to differentiate bacterial infections from other inflammatory diseases. The method is based on the reduction of soluble NBT dye by neutrophils into an insoluble formazan precipitate. If the number of NBT-positive cells is more than 10%, the test is considered positive. 3) Clinical blood test to detect acute phase indicators: an increase in ESR to 50 mm / h or more, leukocytosis with a shift of the leukocyte formula to the left or (in stage II) leukopenia and hypochromic anemia can be detected. Diagnostic value is attached to the detection of histiocytes in the blood taken from the earlobe. Their content of more than 6 in the field of view may indicate in favor of IE. A biochemical blood test shows an increase in the content of fibrinogen, α2-globulins and α-globulins - up to 30-40%. 4) Identification of immunological changes: hypergammaglobulinemia, circulating immune complexes, decrease in complement titer, the appearance of rheumatoid (antiglobulin) factor, increased reaction of imperious transformation of lymphocytes with PHA (phytohemagglutinin) and bacterial antigens, detection of anti-tissue antibodies. 5) Urinalysis is performed to clarify the lesions of various organs and systems, when glomerulonephritis is detected, manifested by proteinuria, cylindruria and hematuria. An increase in the content of bilirubin, transaminases indicates liver damage. 6) A direct diagnostic sign of IE - the presence of vegetation on the heart valves - is detected by echocardiography. Thus, from the whole variety of symptoms, the main and additional ones should be distinguished. The main criteria for the diagnosis of IE: 1) fever with a temperature above 38 ° C with chills; 2) Lukin spots; 3) Osler's nodules; 4) endocarditis on unchanged valves (primary) or against the background of rheumatic and congenital heart defects. infectious myocarditis; 5) multiple arterial thromboembolism, ruptures of mycotic aneurysms with hemorrhages; 6) splenomegaly; 7) positive blood culture; 8) a pronounced positive effect from the use of antibiotics. Additional criteria for the diagnosis of IE: 1) an increase in body temperature up to 38 ° C, chilling; 2) hemorrhages on the skin; 3) rapid weight loss; 4) asymmetric arthritis of small joints of hands, feet; 5) anemization; 6) ESR over 40 mm/h; 7) sharply positive SRV; 8) the presence of rheumatoid factor; 9) α-globulins above 25%; 10) increase in the content of immunoglobulins M, E and A. Differential diagnostics. Although thromboembolism is most often observed in IE, other causes of embolism in the artery of the systemic circulation should not be excluded: transmural myocardial infarction and cardiac aneurysm, idiopathic Abramov-Fiedler myocarditis and atrial fibrillation of various origins, but primarily observed in rheumatic stenosis of the left atrioventricular orifice . Rheumatic and infective endocarditis are of the greatest importance for differential diagnosis (Table 7). Table 7 Differential diagnostic criteria for rheumatic endocarditis and prolonged IE
The characteristic symptoms of IE include an enlarged spleen. However, a large, firm, painless spleen is seen in amyloidosis; soft, painless indicates its septic hyperplasia. Soreness is noted with infarction of the spleen, located subcapsularly. Splenomegaly may be one of the manifestations of portal hypertension in right heart failure. In this case, it is combined with ascites and hepatomegaly. An increase in liver size with prolonged IE is observed quite often. Septic hyperplasia is characterized by relatively small enlargement and soft consistency of the liver. There are fatty degeneration and extremely rarely - liver infarcts. Most often, an increase in the liver is associated with venous congestion with right heart failure. In the absence of ascites, congestion is recognized retrospectively by a decrease in liver size after treatment with cardiac glycosides and diuretics. Treatment. Treatment of IE should be as early and etiotropic as possible, taking into account bacteriological data. Before antibacterial drugs found their widespread use in medical practice, most patients with IE died from infection and its complications. More than 80% are now successfully cured. But for nearly 20%, drug treatment fails and they soon develop heart failure, which is nearly untreatable. In this regard, a combination of conservative and surgical treatment is advisable. For the treatment of IE in any age group, antibiotics are primarily used that have a bactericidal effect on microorganisms, preferably in individualized doses depending on the concentration of the antibiotic in the blood and the sensitivity of the pathogen to it. The drug of first choice is still penicillin. It has low toxicity, which allows it to be used for a long time at relatively high dosages. The daily dose - up to 20 IU is administered intravenously and intramuscularly. However, one should not exclude the fact that in elderly and senile patients, when treated with penicillin and other antibiotics in high doses, a cardiotoxic effect is often observed: the appearance or intensification of heart failure, pain in the heart, tachycardia. When the dose is reduced or the drug is changed, these phenomena stop. With an unknown etiology, treatment begins with high doses of benzylpenicillin intramuscularly or intravenously up to 18-000 units or more, a combination with streptomycin up to 000 g / m per day or aminoglycosides (gentamicin, tobramycin at the rate of 20-000 mg / day) is used. kg per day). In the absence of effect or after determining the pathogen, semi-synthetic penicillins are used (oxacillin, methicillin or ampicillin intramuscularly up to 000 g / day). Cephalosporins are also basic drugs used for the treatment of IE: the most commonly used are claforan, cefamisin (1-4 g/day, intramuscularly and intravenously), as well as zeporin (6-12 g/day) and kefzol (up to 4-10 g intravenously). and etc.). Fusidin has a good anti-staphylococcal effect, in some cases it is effective in the resistance of microorganisms to other antibiotics (10-16 g / day). Antibiotic treatment is prescribed for a long time in a course of 1,5-2 months, until the infection is completely eliminated. After the elimination of the infection, the general condition of the patient improves, the vegetation disappears according to echocardiography and microbiological confirmation. With reduced immunoreactivity of the organism, antibacterial agents are combined with passive immunotherapy (for example, with staphylococcal endocarditis - with antistaphylococcal plasma or antistaphylococcal α-globulin), using immunomodulators (thymalin, T-activin, etc.). To prevent thrombosis, for example, with endocarditis that has developed against the background of angiogenic sepsis, controlled hypocoagulation is created using heparin (20-000 IU intravenously or subcutaneously). For inhibition of proteolytic enzymes, contrical is used (up to 25-000 IU intravenously). When valvular IE contributed to the formation of valvular heart disease or the manifestations of the disease do not disappear despite massive antibiotic therapy, it is advisable to perform surgical treatment. An additional argument in favor of surgical intervention is repeated embolism from the heart valve leaflets destroyed by infection. Sometimes the infection goes beyond the boundaries of the valve ring, while forming abscesses, which is also an indication for surgical treatment. The main goal of the operation is to preserve the patient's own valve. Sometimes they are limited to removing vegetations, suturing ruptures of the valves, etc. If the valve is almost completely destroyed under the influence of infection, it is replaced with an artificial one (prosthesis) using mechanical and biological prostheses. Prevention. Prevention of IE consists of timely sanitation of chronic foci of infection in the oral cavity, tonsils, nasopharynx, paranasal sinuses, and the use of active antibacterial therapy for acute streptococcal and staphylococcal diseases (angina, etc.). It is recommended to harden the body. All patients with valvular heart disease, as well as with valve prostheses, should take antibiotics prophylactically the day before and shortly after any intervention, after which an infection can enter the bloodstream. Dispensary observation of persons who have had acute streptococcal, staphylococcal infections is necessary. Author: Mostovaya O.S. << Back: Diseases of the cardiovascular system. Restrictive cardiomyopathy >> Forward: Respiratory diseases. Bronchial asthma
▪ International economic relations. Lecture notes ▪ Teria of the organization. Crib ▪ Obstetrics and gynecology. Crib
The existence of an entropy rule for quantum entanglement has been proven
09.05.2024 Mini air conditioner Sony Reon Pocket 5
09.05.2024 Energy from space for Starship
08.05.2024
▪ Marine fish are toxic and carcinogenic ▪ The composition of the intestinal microflora ▪ Samsung has released a mobile phone with a hard drive
▪ site section And then an inventor (TRIZ) appeared. Article selection ▪ article To the fullest (full) to do something. Popular expression ▪ article How Many Languages Do Nigerians Speak? Detailed answer ▪ article Musk root. Legends, cultivation, methods of application ▪ article Miracle album. Focus Secret
Home page | Library | Articles | Website map | Site Reviews
www.diagram.com.ua |



 See other articles Section
See other articles Section 